This article is about the male prostate gland. For the equivalent female prostate gland, see Skene’s gland. For the journal, see The Prostate.
| Prostate | |
|---|---|
 |
|
| Details | |
| Precursor | Endodermic evaginations of the urethra |
| Artery | Internal pudendal artery, inferior vesical artery, and middle rectal artery |
| Vein | Prostatic venous plexus, pudendal plexus, vesical plexus, internal iliac vein |
| Nerve | Inferior hypogastric plexus |
| Lymph | internal iliac lymph nodes |
| Identifiers | |
| Latin | Prostata |
| MeSH | D011467 |
| TA98 | A09.3.08.001 |
| TA2 | 3637 |
| FMA | 9600 |
| Anatomical terminology
[edit on Wikidata] |
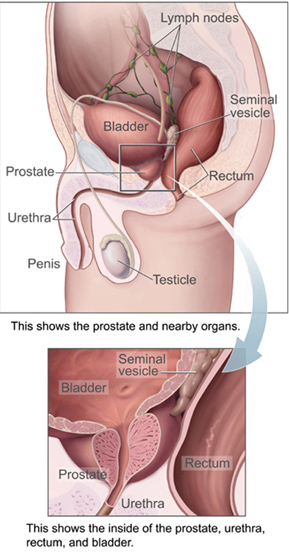
The prostate is both an accessory gland of the male reproductive system and a muscle-driven mechanical switch between urination and ejaculation. It is found in all male mammals.[1] It differs between species anatomically, chemically, and physiologically. Anatomically, the prostate is found below the bladder, with the urethra passing through it. It is described in gross anatomy as consisting of lobes and in microanatomy by zone. It is surrounded by an elastic, fibromuscular capsule and contains glandular tissue as well as connective tissue.
The prostate glands produce and contain fluid that forms part of semen, the substance emitted during ejaculation as part of the male sexual response. This prostatic fluid is slightly alkaline, milky or white in appearance. The alkalinity of semen helps neutralize the acidity of the vaginal tract, prolonging the lifespan of sperm. The prostatic fluid is expelled in the first part of ejaculate, together with most of the sperm, because of the action of smooth muscle tissue within the prostate. In comparison with the few spermatozoa expelled together with mainly seminal vesicular fluid, those in prostatic fluid have better motility, longer survival, and better protection of genetic material.
Disorders of the prostate include enlargement, inflammation, infection, and cancer. The word prostate comes from Ancient Greek προστάτης, prostátēs, meaning «one who stands before», «protector», «guardian», with the term originally used to describe the seminal vesicles.
Structure[edit]
The prostate is a gland of the male reproductive system. In adults, it is about the size of a walnut,[2] and has an average weight of about 11 grams, usually ranging between 7 and 16 grams.[3] The prostate is located in the pelvis. It sits below the urinary bladder and surrounds the urethra. The part of the urethra passing through it is called the prostatic urethra, which joins with the two ejaculatory ducts.[2] The prostate is covered in a surface called the prostatic capsule or prostatic fascia.[4]
The internal structure of the prostate has been described using both lobes and zones.[5][2] Because of the variation in descriptions and definitions of lobes, the zone classification is used more predominantly.[2]
The prostate has been described as consisting of three or four zones.[2][4] Zones are more typically able to be seen on histology, or in medical imaging, such as ultrasound or MRI.[2][5] The zones are:
| Name | Fraction of adult gland[2] | Description |
| Peripheral zone (PZ) | 70% | The back of the gland that surrounds the distal urethra and lies beneath the capsule. About 70–80% of prostatic cancers originate from this zone of the gland.[6][7] |
| Central zone (CZ) | 20% | This zone surrounds the ejaculatory ducts.[2] The central zone accounts for roughly 2.5% of prostate cancers; these cancers tend to be more aggressive and more likely to invade the seminal vesicles.[8] |
| Transition zone (TZ) | 5% | The transition zone surrounds the proximal urethra.[2] ~10–20% of prostate cancers originate in this zone. It is the region of the prostate gland that grows throughout life and causes the disease of benign prostatic enlargement.[6][7] |
| Anterior fibro-muscular zone (or stroma) | N/A | This area, not always considered a zone,[4] is usually devoid of glandular components and composed only, as its name suggests, of muscle and fibrous tissue.[2] |
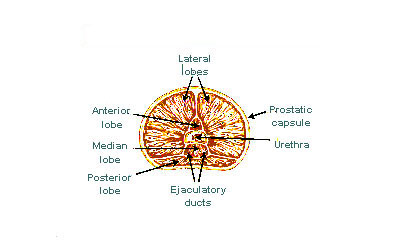
The «lobe» classification describes lobes that, while originally defined in the fetus, are also visible in gross anatomy, including dissection and when viewed endoscopically.[5][4] The five lobes are the anterior lobe or isthmus, the posterior lobe, the right and left lateral lobes, and the middle or median lobe.
-

Lobes of prostate
-

Zones of prostate

Inside of the prostate, adjacent and parallel to the prostatic urethra, there are two longitudinal muscle systems. On the front side (ventrally) runs the urethral dilator (musculus dilatator urethrae), on the backside (dorsally) runs the muscle switching the urethra into the ejaculatory state (musculus ejaculatorius).[9]
Blood and lymphatic vessels[edit]
The prostate receives blood through the inferior vesical artery, internal pudendal artery, and middle rectal arteries. These vessels enter the prostate on its outer posterior surface where it meets the bladder, and travel forward to the apex of the prostate.[4] Both the inferior vesical and the middle rectal arteries often arise together directly from the internal iliac arteries. On entering the bladder, the inferior vesical artery splits into a urethral branch, supplying the urethral prostate; and a capsular branch, which travels around the capsule and has smaller branches which perforate into the prostate.[4]
The veins of the prostate form a network – the prostatic venous plexus, primarily around its front and outer surface.[4] This network also receives blood from the deep dorsal vein of the penis, and is connected via branches to the vesical plexus and internal pudendal veins.[4] Veins drain into the vesical and then internal iliac veins.[4]
The lymphatic drainage of the prostate depends on the positioning of the area. Vessels surrounding the vas deferens, some of the vessels in the seminal vesicle, and a vessel from the posterior surface of the prostate drain into the external iliac lymph nodes.[4] Some of the seminal vesicle vessels, prostatic vessels, and vessels from the anterior prostate drain into internal iliac lymph nodes.[4] Vessels of the prostate itself also drain into the obturator and sacral lymph nodes.[4]

Microanatomy[edit]

The prostate consists of glandular and connective tissue.[2] Tall column-shaped cells form the lining (the epithelium) of the glands.[2] These form one layer or may be pseudostratified.[4] The epithelium is highly variable and areas of low cuboidal or flat cells can also be present, with transitional epithelium in the outer regions of the longer ducts.[10] The glands are formed as many follicles, which in drain into canals and subsequently 12–20 main ducts, These in turn drain into the urethra as it passes through the prostate.[4] There are also a small amount of flat cells, which sit next to the basement membranes of glands, and act as stem cells.[2]
The connective tissue of the prostate is made up of fibrous tissue and smooth muscle.[2] The fibrous tissue separates the gland into lobules.[2] It also sits between the glands and is composed of randomly orientated smooth-muscle bundles that are continuous with the bladder.[11]
Over time, thickened secretions called corpora amylacea accumulate in the gland.[2]
-

Microscopic glands of the prostate

Gene and protein expression[edit]
About 20,000 protein coding genes are expressed in human cells and almost 75% of these genes are expressed in the normal prostate.[12][13] About 150 of these genes are more specifically expressed in the prostate, with about 20 genes being highly prostate specific.[14] The corresponding specific proteins are expressed in the glandular and secretory cells of the prostatic gland and have functions that are important for the characteristics of semen, including prostate-specific proteins, such as the prostate specific antigen (PSA), and the Prostatic acid phosphatase.[15]
Development[edit]
In the developing embryo, at the hind end lies an inpouching called the cloaca. This, over the fourth to the seventh week, divides into a urogenital sinus and the beginnings of the anal canal, with a wall forming between these two inpouchings called the urorectal septum.[16] The urogenital sinus divides into three parts, with the middle part forming the urethra; the upper part is largest and becomes the urinary bladder, and the lower part then changes depending on the biological sex of the embryo.[16]
The prostatic part of the urethra develops from the middle, pelvic, part of the urogenital sinus, which is of endodermal origin.[17] Around the end of the third month of embryonic life, outgrowths arise from the prostatic part of the urethra and grow into the surrounding mesenchyme.[17] The cells lining this part of the urethra differentiate into the glandular epithelium of the prostate.[17] The associated mesenchyme differentiates into the dense connective tissue and the smooth muscle of the prostate.[18]
Condensation of mesenchyme, urethra, and Wolffian ducts gives rise to the adult prostate gland, a composite organ made up of several tightly fused glandular and non-glandular components. To function properly, the prostate needs male hormones (androgens), which are responsible for male sex characteristics. The main male hormone is testosterone, which is produced mainly by the testicles. It is dihydrotestosterone (DHT), a metabolite of testosterone, that predominantly regulates the prostate. The prostate gland enlarges over time, until the fourth decade of life.[4]
Function[edit]
The prostate secretes fluid which becomes part of semen. Semen is the fluid emitted (ejaculated) by males during the sexual response.[19] When sperm is emitted, it is transmitted from the vas deferens into the male urethra via the ejaculatory ducts, which lie within the prostate gland.[19] Ejaculation is the expulsion of semen from the urethra.[19] Semen is moved into the urethra following contractions of the smooth muscle of the vas deferens and seminal vesicles, following stimulation, primarily of the glans penis. Stimulation sends nerve signals via the internal pudendal nerves to the upper lumbar spine; the nerve signals causing contraction act via the hypogastric nerves.[19] After traveling into the urethra, the seminal fluid is ejaculated by contraction of the bulbocavernosus muscle.[19] The secretions of the prostate include proteolytic enzymes, prostatic acid phosphatase, fibrinolysin, zinc, and prostate-specific antigen.[4] Together with the secretions from the seminal vesicles, these form the major fluid part of semen.[4]
It is possible for some men to achieve orgasm solely through stimulation of the prostate gland, such as via prostate massage or anal intercourse.[20][21] This has led to the area of the rectal wall adjacent to the prostate to be popularly referred by the anatomically incorrect term, the «male G-spot».[22]
The prostate’s changes of shape, which facilitate the mechanical switch between urination and ejaculation, are mainly driven by the two longitudinal muscle systems running along the prostatic urethra. These are the urethral dilator (musculus dilatator urethrae) on the urethra’s front side, which contracts during urination and thereby shortens and tilts the prostate in its vertical dimension thus widening the prostatic section of the urethral tube,[23][24] and the muscle switching the urethra into the ejaculatory state (musculus ejaculatorius) on its backside.[9]
In case of an operation, e.g. because of benign prostatic hyperplasia (BPH), damaging or sparing of these two muscle systems varies considerably depending on the choice of operation type and details of the procedure of the chosen technique. The effects on postoperational urination and ejaculation vary correspondingly.[25] (See also: Surgery for benign prostatic hyperplasia).
Clinical significance[edit]
Inflammation[edit]

Micrograph showing an inflamed prostate gland, found in prostatitis. A large amount of darker cells, representing leukocytes, can be seen. An area without inflammation is seen on the left of the image. H&E stain.
Prostatitis is inflammation of the prostate gland. It can be caused by infection with bacteria, or other noninfective causes. Inflammation of the prostate can cause painful urination or ejaculation, groin pain, difficulty passing urine, or constitutional symptoms such as fever or tiredness.[26] When inflamed, the prostate becomes enlarged and is tender when touched during digital rectal examination. The bacteria responsible for the infection may be detected by a urine culture.[26]
Acute prostatitis and chronic bacterial prostatitis are treated with antibiotics.[26] Chronic non-bacterial prostatitis, or male chronic pelvic pain syndrome is treated by a large variety of modalities including the medications alpha blockers, nonsteroidal antiinflammatories and amitriptyline,[26] antihistamines, and other anxiolytics.[27] Other treatments that are not medications may include physical therapy,[28] psychotherapy, nerve modulators, and surgery. More recently, a combination of trigger point and psychological therapy has proved effective for category III prostatitis as well.[27]
Enlarged prostate[edit]
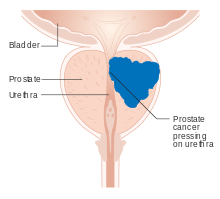
A diagram of prostate cancer pressing on the urethra, which can cause symptoms

An enlarged prostate is called prostatomegaly, with benign prostatic hyperplasia (BPH) being the most common cause. BPH refers to an enlargement of the prostate due to an increase in the number of cells that make up the prostate (hyperplasia) from a cause that is not a malignancy. It is very common in older men.[26] It is often diagnosed when the prostate has enlarged to the point where urination becomes difficult. Symptoms include needing to urinate often (urinary frequency) or taking a while to get started (urinary hesitancy). If the prostate grows too large, it may constrict the urethra and impede the flow of urine, making urination painful and difficult, or in extreme cases completely impossible, causing urinary retention.[26] Over time, chronic retention may cause the bladder to become larger and cause a backflow of urine into the kidneys (hydronephrosis).[26]
BPH can be treated with medication, a minimally invasive procedure or, in extreme cases, surgery that removes the prostate. In general, treatment often begins with an alpha-1 adrenergic receptor antagonist medication such as tamsulosin, which reduces the tone of the smooth muscle found in the urethra that passes through the prostate, making it easier for urine to pass through.[26] For people with persistent symptoms, procedures may be considered. The surgery most often used in such cases is transurethral resection of the prostate,[26] in which an instrument is inserted through the urethra to remove prostate tissue that is pressing against the upper part of the urethra and restricting the flow of urine. Minimally invasive procedures include transurethral needle ablation of the prostate and transurethral microwave thermotherapy.[29] These outpatient procedures may be followed by the insertion of a temporary stent, to allow normal voluntary urination, without exacerbating irritative symptoms.[30]
Cancer[edit]
Prostate cancer is one of the most common cancers affecting older men in the UK, US, Northern Europe and Australia, and a significant cause of death for elderly men worldwide.[31] Often, a person does not have symptoms; when they do occur, symptoms may include urinary frequency, urgency, hesitation and other symptoms associated with BPH. Uncommonly, such cancers may cause weight loss, retention of urine, or symptoms such as back pain due to metastatic lesions that have spread outside of the prostate.[26]
A digital rectal examination and the measurement of a prostate-specific antigen (PSA) level are usually the first investigations done to check for prostate cancer. PSA values are difficult to interpret, because a high value might be present in a person without cancer, and a low value can be present in someone with cancer.[26] The next form of testing is often the taking of a biopsy to assess for tumour activity and invasiveness.[26] Because of the significant risk of overdiagnosis with widespread screening in the general population, prostate cancer screening is controversial.[32] If a tumour is confirmed, medical imaging such as an MRI or bone scan may be done to check for the presence of tumour metastases in other parts of the body.[26]
Prostate cancer that is only present in the prostate is often treated with either surgical removal of the prostate or with radiotherapy or by the insertion of small radioactive particles of iodine-125 or palladium-103, called brachytherapy.[33][26] Cancer that has spread to other parts of the body is usually treated also with hormone therapy, to deprive a tumour of sex hormones (androgens) that stimulate proliferation. This is often done through the use of GnRH analogues or agents (such as bicalutamide) that block the receptors that androgens act on; occasionally, surgical removal of the testes may be done instead.[26] Cancer that does not respond to hormonal treatment, or that progresses after treatment, might be treated with chemotherapy such as docetaxel. Radiotherapy may also be used to help with pain associated with bony lesions.[26]
Sometimes, the decision may be made not to treat prostate cancer. If a cancer is small and localised, the decision may be made to monitor for cancer activity at intervals («active surveillance») and defer treatment.[26] If a person, because of frailty or other medical conditions or reasons, has a life expectancy less than ten years, then the impacts of treatment may outweigh any perceived benefits.[26]
Surgery[edit]
Surgery to remove the prostate is called prostatectomy, and is usually done as a treatment for cancer limited to the prostate, or prostatic enlargement.[34] When it is done, it may be done as open surgery or as laparoscopic (keyhole) surgery.[34] These are done under general anaesthetic.[35] Usually the procedure for cancer is a radical prostatectomy, which means that the seminal vesicles are removed and vas deferens is also tied off.[34] Part of the prostate can also be removed from within the urethra, called transurethral resection of the prostate (TURP).[34] Open surgery may involve a cut that is made in the perineum, or via an approach that involves a cut down the midline from the belly button to the pubic bone.[34] Open surgery may be preferred if there is a suspicion that lymph nodes are involved and they need to be removed or biopsied during a procedure.[34] A perineal approach will not involve lymph node removal and may result in less pain and a faster recovery following an operation.[34] A TURP procedure uses a tube inserted into the urethra via the penis and some form of heat, electricity or laser to remove prostate tissue.[34]
The whole prostate can be removed. Complications that might develop because of surgery include urinary incontinence and erectile dysfunction because of damage to nerves during the operation, particularly if a cancer is very close to nerves.[34][35] Ejaculation of semen will not occur during orgasm if the vas deferens are tied off and seminal vesicles removed, such as during a radical prosatectomy.[34] This will mean a man becomes infertile.[34] Sometimes, orgasm may not be able to occur or may be painful. The penis length may change if the part of the urethra within the prostate is also removed.[34] General complications due to surgery can also develop, such as infections, bleeding, inadvertent damage to nearby organs or within the abdomen, and the formation of blood clots.[34]
History[edit]
The prostate was first formally identified by Venetian anatomist Niccolò Massa in Anatomiae libri introductorius (Introduction to Anatomy) 1536 and illustrated by Flemish anatomist Andreas Vesalius in Tabulae anatomicae sex (six anatomical tables) in 1538.[36][5] Massa described it as a «glandular flesh upon which rests the neck of the bladder,» and Vesalius as a «glandular body».[37] The first time a word similar to ‘prostate’ was used to describe the gland is credited to André du Laurens in 1600, who described it as a term already in use by anatomists at the time.[37][5] The term was however used at least as early as 1549 by French surgeon Ambroise Pare.[5]
At the time, Du Laurens was describing what was considered to be a pair of organs (not the single two-lobed organ), and the Latin term prostatae that was used was a mistranslation of the term for the Ancient Greek word used to describe the seminal vesicles, parastatai;[37] although it has been argued that surgeons in Ancient Greece and Rome must have at least seen the prostate as an anatomical entity.[5] The term prostatae was taken rather than the grammatically correct prostator (singular) and prostatores (plural) because the gender of the Ancient Greek term was taken as female, when it was in fact male.[37]
The fact that the prostate was one and not two organs was an idea popularised throughout the early 18th century, as was the English language term used to describe the organ, prostate,[37] attributed to William Cheselden.[38] A monograph, «Practical observations on the treatment of the diseases of the prostate gland» by Everard Home in 1811, was important in the history of the prostate by describing and naming anatomical parts of the prostate, including the median lobe.[37] The idea of the five lobes of the prostate was popularized following anatomical studies conducted by American urologist Oswald Lowsley in 1912.[5][38] John E. McNeal first proposed the idea of «zones» in 1968; McNeal found that the relatively homogeneous cut surface of an adult prostate in no way resembled «lobes» and thus led to the description of «zones».[39]
Prostate cancer was first described in a speech to the Medical and Chiurgical Society of London in 1853 by surgeon John Adams[40][41] and increasingly described by the late 19th century.[42] Prostate cancer was initially considered a rare disease, probably because of shorter life expectancies and poorer detection methods in the 19th century. The first treatments of prostate cancer were surgeries to relieve urinary obstruction.[43] Samuel David Gross has been credited with the first mention of a prostatectomy, as «too absurd to be seriously entertained»[44][42] The first removal for prostate cancer (radical perineal prostatectomy) was first performed in 1904 by Hugh H. Young at Johns Hopkins Hospital;[45][42] partial removal of the gland was conducted by Theodore Billroth in 1867.[38]
Transurethral resection of the prostate (TURP) replaced radical prostatectomy for symptomatic relief of obstruction in the middle of the 20th century because it could better preserve penile erectile function. Radical retropubic prostatectomy was developed in 1983 by Patrick Walsh.[46] In 1941, Charles B. Huggins published studies in which he used estrogen to oppose testosterone production in men with metastatic prostate cancer. This discovery of «chemical castration» won Huggins the 1966 Nobel Prize in Physiology or Medicine.[47]
The role of the gonadotropin-releasing hormone (GnRH) in reproduction was determined by Andrzej W. Schally and Roger Guillemin, who both won the 1977 Nobel Prize in Physiology or Medicine for this work. GnRH receptor agonists, such as leuprorelin and goserelin, were subsequently developed and used to treat prostate cancer.[48][49] Radiation therapy for prostate cancer was first developed in the early 20th century and initially consisted of intraprostatic radium implants. External beam radiotherapy became more popular as stronger X-ray radiation sources became available in the middle of the 20th century. Brachytherapy with implanted seeds (for prostate cancer) was first described in 1983.[50] Systemic chemotherapy for prostate cancer was first studied in the 1970s. The initial regimen of cyclophosphamide and 5-fluorouracil was quickly joined by multiple regimens using a host of other systemic chemotherapy drugs.[51]
Other animals[edit]
The prostate is found only in mammals.[52] The prostate glands of male marsupials are proportionally larger than those of placental mammals.[53] The presence of a functional prostate in monotremes is controversial, and if monotremes do possess functional prostates, they may not make the same contribution to semen as in other mammals.[54]
The structure of the prostate varies, ranging from tubuloalveolar (as in humans) to branched tubular. The gland is particularly well developed in dogs, foxes and boars, though in other mammals, such as bulls, it can be small and inconspicuous.[55][56][57] In other animals, such as marsupials[58][59] and small ruminants, the prostate is disseminate, meaning not specifically localisable as a distinct tissue, but present throughout the relevant part of the urethra; in other animals, such as red deer and American elk, it may be present as a specific organ and in a disseminate form.[60] In some marsupial species, the size of the prostate gland changes seasonally.[61] The prostate is the only accessory gland that occurs in male dogs.[62] Dogs can produce in one hour as much prostatic fluid as a human can in a day. They excrete this fluid along with their urine to mark their territory.[63] Additionally, dogs are the only species apart from humans seen to have a significant incidence of prostate cancer.[64] In cetaceans (whales, dolphins, porpoises) the prostate is composed of diffuse urethral glands[65] and is surrounded by a very powerful compressor muscle.[66]
The prostate gland originates with tissues in the urethral wall.[citation needed] This means the urethra, a compressible tube used for urination, runs through the middle of the prostate. This leads to an evolutionary design fault for some mammals, including human males. The prostate is prone to infection and enlargement later in life, constricting the urethra so urinating becomes slow and painful.[67]
Prostatic secretions vary among species. They are generally composed of simple sugars and are often slightly alkaline.[68]
Skene’s gland[edit]
Because the Skene’s gland and the male prostate act similarly by secreting prostate-specific antigen (PSA), which is an ejaculate protein produced in males, and of prostate-specific acid phosphatase, the Skene’s gland is sometimes referred to as the «female prostate».[69][70] Although it is homologous to the male prostate (developed from the same embryological tissues),[71][72] various aspects of its development in relation to the male prostate are widely unknown and a matter of research.[73]
See also[edit]
- Ejaculatory duct
- Seminal vesicles
- Prostate evolution in monotreme mammals
References[edit]
Citations[edit]
- ^ Vásquez, Bélgica (2014-03-01). «Morphological Characteristics of Prostate in Mammals». International Journal of Medical and Surgical Sciences. 1 (1): 63–72. doi:10.32457/ijmss.2014.010. ISSN 0719-532X.
- ^ a b c d e f g h i j k l m n o p Young, Barbara; O’Dowd, Geraldine; Woodford, Phillip (2013). Wheater’s functional histology: a text and colour atlas (6th ed.). Philadelphia: Elsevier. pp. 347–8. ISBN 9780702047473.
- ^ Leissner KH, Tisell LE (1979). «The weight of the human prostate». Scand. J. Urol. Nephrol. 13 (2): 137–42. doi:10.3109/00365597909181168. PMID 90380.
- ^ a b c d e f g h i j k l m n o p q Standring, Susan, ed. (2016). «Prostate». Gray’s anatomy : the anatomical basis of clinical practice (41st ed.). Philadelphia. pp. 1266–1270. ISBN 9780702052309. OCLC 920806541.
- ^ a b c d e f g h Goddard, Jonathan Charles (January 2019). «The history of the prostate, part one: say what you see». Trends in Urology & Men’s Health. 10 (1): 28–30. doi:10.1002/tre.676.
- ^ a b «Basic Principles: Prostate Anatomy» Archived 2010-10-15 at the Wayback Machine. Urology Match. Www.urologymatch.com. Web. 14 June 2010.
- ^ a b «Prostate Cancer Information from the Foundation of the Prostate Gland.» Prostate Cancer Treatment Guide. Web. 14 June 2010.
- ^ Cohen RJ, Shannon BA, Phillips M, Moorin RE, Wheeler TM, Garrett KL (2008). «Central zone carcinoma of the prostate gland: a distinct tumor type with poor prognostic features». The Journal of Urology. 179 (5): 1762–7, discussion 1767. doi:10.1016/j.juro.2008.01.017. PMID 18343454.
- ^ a b Michael Schünke, Erik Schulte, Udo Schumacher: PROMETHEUS Innere Organe. LernAtlas Anatomie, vol 2: Innere Organe, Thieme Verlag, Stuttgart/Germany 2012, ISBN 9783131395337, p. 298, PDF.
- ^ «Prostate Gland Development». ana.ed.ac.uk. Archived from the original on 2003-04-30. Retrieved 2011-08-03.
- ^ «Prostate». webpath.med.utah.edu. Retrieved 2019-11-17.
- ^ «The human proteome in prostate – The Human Protein Atlas». www.proteinatlas.org. Retrieved 2017-09-26.
- ^ Uhlén, Mathias; Fagerberg, Linn; Hallström, Björn M.; Lindskog, Cecilia; Oksvold, Per; Mardinoglu, Adil; Sivertsson, Åsa; Kampf, Caroline; Sjöstedt, Evelina (2015-01-23). «Tissue-based map of the human proteome». Science. 347 (6220): 1260419. doi:10.1126/science.1260419. ISSN 0036-8075. PMID 25613900. S2CID 802377.
- ^ O’Hurley, Gillian; Busch, Christer; Fagerberg, Linn; Hallström, Björn M.; Stadler, Charlotte; Tolf, Anna; Lundberg, Emma; Schwenk, Jochen M.; Jirström, Karin (2015-08-03). «Analysis of the Human Prostate-Specific Proteome Defined by Transcriptomics and Antibody-Based Profiling Identifies TMEM79 and ACOXL as Two Putative, Diagnostic Markers in Prostate Cancer». PLOS ONE. 10 (8): e0133449. Bibcode:2015PLoSO..1033449O. doi:10.1371/journal.pone.0133449. ISSN 1932-6203. PMC 4523174. PMID 26237329.
- ^ Kong, HY; Byun, J (January 2013). «Emerging roles of human prostatic Acid phosphatase». Biomolecules & Therapeutics. 21 (1): 10–20. doi:10.4062/biomolther.2012.095. PMC 3762301. PMID 24009853.
- ^ a b Sadley, TW (2019). «Bladder and urethra». Langman’s medical embryology (14th ed.). Philadelphia: Wolters Kluwer. pp. 263–66. ISBN 9781496383907.
- ^ a b c Sadley, TW (2019). Langman’s medical embryology (14th ed.). Philadelphia: Wolters Kluwer. pp. 265–6. ISBN 9781496383907.
- ^ Moore, Keith L.; Persaud, T. V. N.; Torchia, Mark G. (2008). Before We are Born: Essentials of Embryology and Birth Defects (7th ed.). ISBN 978-1-4160-3705-7.
- ^ a b c d e Barrett, Kim E. (2019). Ganong’s review of medical physiology. Barman, Susan M.,, Brooks, Heddwen L.,, Yuan, Jason X.-J. (26th ed.). New York. pp. 411, 415. ISBN 9781260122404. OCLC 1076268769.
- ^ Rosenthal, Martha (2012). Human Sexuality: From Cells to Society. Cengage Learning. pp. 133–135. ISBN 978-0618755714. Retrieved September 17, 2012.
- ^ Komisaruk, Barry R.; Whipple, Beverly; Nasserzadeh, Sara & Beyer-Flores, Carlos (2009). The Orgasm Answer Guide. JHU Press. pp. 108–109. ISBN 978-0-8018-9396-4. Retrieved 6 November 2011.
- ^ Levin, R. J. (2018). «Prostate-induced orgasms: A concise review illustrated with a highly relevant case study». Clinical Anatomy. 31 (1): 81–85. doi:10.1002/ca.23006. PMID 29265651.
- ^ Hocaoglu Y, Roosen A, Herrmann K, Tritschler S, Stief C, Bauer RM (2012). «Real-time magnetic resonance imaging (MRI): anatomical changes during physiological voiding in men». BJU Int. 109 (2): 234–9. doi:10.1111/j.1464-410X.2011.10255.x. PMID 21736694.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ^ Hocaoglu Y, Herrmann K, Walther S, Hennenberg M, Gratzke C, Bauer R; et al. (2013). «Contraction of the anterior prostate is required for the initiation of micturition». BJU Int. 111 (7): 1117–23. doi:10.1111/j.1464-410X.2012.11698.x. PMID 23356864.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ^ Lebdai S, Chevrot A, Doizi S, Pradere B, Delongchamps NB, Benchikh A; et al. (2019). «Do patients have to choose between ejaculation and miction? A systematic review about ejaculation preservation technics for benign prostatic obstruction surgical treatment» (PDF). World J Urol. 37 (2): 299–308. doi:10.1007/s00345-018-2368-6. PMID 29967947. S2CID 49556196. Archived from the original (PDF) on 2021-08-11. Retrieved 2020-11-16.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ^ a b c d e f g h i j k l m n o p q r Davidson’s 2018, pp. 437–9.
- ^ a b Anderson RU, Wise D, Sawyer T, Chan CA (2006). «Sexual dysfunction in men with chronic prostatitis/chronic pelvic pain syndrome: improvement after trigger point release and paradoxical relaxation training». J. Urol. 176 (4 Pt 1): 1534–8, discussion 1538–9. CiteSeerX 10.1.1.383.7495. doi:10.1016/j.juro.2006.06.010. PMID 16952676.
- ^ «Physical Therapy Treatment for Prostatitis/chronic pelvic pain syndrome». 2014. Retrieved 2014-10-22.
- ^ Christensen, TL; Andriole, GL (February 2009). «Benign Prostatic Hyperplasia: Current Treatment Strategies». Consultant. 49 (2).
- ^ Dineen MK, Shore ND, Lumerman JH, Saslawsky MJ, Corica AP (2008). «Use of a Temporary Prostatic Stent After Transurethral Microwave Thermotherapy Reduced Voiding Symptoms and Bother Without Exacerbating Irritative Symptoms». J. Urol. 71 (5): 873–877. doi:10.1016/j.urology.2007.12.015. PMID 18374395.
- ^ Rawla P (April 2019). «Epidemiology of Prostate Cancer». World J Oncol (Review). 10 (2): 63–89. doi:10.14740/wjon1191. PMC 6497009. PMID 31068988.
- ^ Sandhu, Gurdarshan S.; Andriole, Gerald L. (September 2012). «Overdiagnosis of Prostate Cancer». Journal of the National Cancer Institute. Monographs. 2012 (45): 146–151. doi:10.1093/jncimonographs/lgs031. ISSN 1052-6773. PMC 3540879. PMID 23271765.
- ^ «What is Brachytherapy?». American Brachytherapy Society. Retrieved 8 August 2020.
- ^ a b c d e f g h i j k l m «Surgery for Prostate Cancer». www.cancer.org. The American Cancer Society medical and editorial content team. 1 August 2019. Retrieved 8 August 2020.
- ^ a b «Surgery to remove your prostate gland | Prostate cancer | Cancer Research UK». www.cancerresearchuk.org. Cancer Research UK. 18 Jun 2019. Retrieved 8 August 2020.
- ^ Ghabili, Kamyar; Tosoian, Jeffrey J.; Schaeffer, Edward M.; Pavlovich, Christian P.; Golzari, Samad E.J.; Khajir, Ghazal; Andreas, Darian; Benzon, Benjamin; Vuica-Ross, Milena; Ross, Ashley E. (November 2016). «The History of Prostate Cancer From Antiquity: Review of Paleopathological Studies». Urology. 97: 8–12. doi:10.1016/j.urology.2016.08.032. PMID 27591810.
- ^ a b c d e f Josef Marx, Franz; Karenberg, Axel (1 February 2009). «History of the Term Prostate». The Prostate. 69 (2): 208–213. doi:10.1002/pros.20871. PMID 18942121. S2CID 44922919.
- ^ a b c Young, Robert H; Eble, John N (January 2019). «The history of urologic pathology: an overview». Histopathology. 74 (1): 184–212. doi:10.1111/his.13753. PMID 30565309. S2CID 56476748.
- ^ Myers, Robert P (2000). «Structure of the adult prostate from a clinician’s standpoint». Clinical Anatomy. 13 (3): 214–5. doi:10.1002/(SICI)1098-2353(2000)13:3<214::AID-CA10>3.0.CO;2-N. PMID 10797630. S2CID 33861863.
- ^ Adams J (1853). «The case of scirrhous of the prostate gland with corresponding affliction of the lymphatic glands in the lumbar region and in the pelvis». Lancet. 1 (1547): 393–94. doi:10.1016/S0140-6736(02)68759-8.
- ^ Ghabili K, Tosoian JJ, Schaeffer EM, Pavlovich CP, Golzari SE, Khajir G, Andreas D, Benzon B, Vuica-Ross M, Ross AE (November 2016). «The History of Prostate Cancer From Antiquity: Review of Paleopathological Studies». Urology. 97: 8–12. doi:10.1016/j.urology.2016.08.032. PMID 27591810.
- ^ a b c Nahon, I; Waddington, G; Dorey, G; Adams, R (2011). «The history of urologic surgery: from reeds to robotics». Urologic Nursing. 31 (3): 173–80. doi:10.7257/1053-816X.2011.31.3.173. PMID 21805756.
- ^ Lytton B (June 2001). «Prostate cancer: a brief history and the discovery of hormonal ablation treatment». The Journal of Urology. 165 (6 Pt 1): 1859–62. doi:10.1016/S0022-5347(05)66228-3. PMID 11371867.
- ^ Samuel David Gross (1851). A Practical Treatise On the Diseases and Injuries of the Urinary Bladder, the Prostate Gland, and the Urethra. Philadelphia: Blanchard and Lea.
«The idea of extirpating the entire gland is, indeed, too absurd to be seriously entertained… Excision of the middle lobe would be far less objectionable»
- ^ Young HH (1905). «Four cases of radical prostatectomy». Johns Hopkins Bull. 16.
- ^ Walsh PC, Lepor H, Eggleston JC (1983). «Radical prostatectomy with preservation of sexual function: anatomical and pathological considerations». The Prostate. 4 (5): 473–85. doi:10.1002/pros.2990040506. PMID 6889192. S2CID 30740301.
- ^ Huggins CB, Hodges CV (1941). «Studies on prostate cancer: 1. The effects of castration, of estrogen and androgen injection on serum phosphatases in metastatic carcinoma of the prostate». Cancer Res. 1 (4): 293. Archived from the original on 2017-06-30.
- ^ Schally AV, Kastin AJ, Arimura A (November 1971). «Hypothalamic follicle-stimulating hormone (FSH) and luteinizing hormone (LH)-regulating hormone: structure, physiology, and clinical studies». Fertility and Sterility. 22 (11): 703–21. doi:10.1016/S0015-0282(16)38580-6. PMID 4941683.
- ^ Tolis G, Ackman D, Stellos A, Mehta A, Labrie F, Fazekas AT, et al. (March 1982). «Tumor growth inhibition in patients with prostatic carcinoma treated with luteinizing hormone-releasing hormone agonists». Proceedings of the National Academy of Sciences of the United States of America. 79 (5): 1658–62. Bibcode:1982PNAS…79.1658T. doi:10.1073/pnas.79.5.1658. PMC 346035. PMID 6461861.
- ^ Denmeade SR, Isaacs JT (May 2002). «A history of prostate cancer treatment». Nature Reviews. Cancer. 2 (5): 389–96. doi:10.1038/nrc801. PMC 4124639. PMID 12044015.
- ^ Scott WW, Johnson DE, Schmidt JE, Gibbons RP, Prout GR, Joiner JR, et al. (December 1975). «Chemotherapy of advanced prostatic carcinoma with cyclophosphamide or 5-fluorouracil: results of first national randomized study». The Journal of Urology. 114 (6): 909–11. doi:10.1016/S0022-5347(17)67172-6. PMID 1104900.
- ^ Marker, Paul C; Donjacour, Annemarie A; Dahiya, Rajvir; Cunha, Gerald R (January 2003). «Hormonal, cellular, and molecular control of prostatic development». Developmental Biology. 253 (2): 165–174. doi:10.1016/s0012-1606(02)00031-3. PMID 12645922.
- ^ Hugh Tyndale-Biscoe; Marilyn Renfree (30 January 1987). Reproductive Physiology of Marsupials. Cambridge University Press. ISBN 978-0-521-33792-2.
- ^ Temple-Smith, P; Grant, T (2001). «Uncertain breeding: a short history of reproduction in monotremes». Reproduction, Fertility, and Development. 13 (7–8): 487–97. doi:10.1071/rd01110. PMID 11999298.
- ^ Sherwood, Lauralee; Klandorf, Hillar; Yancey, Paul (January 2012). Animal Physiology: From Genes to Organisms. p. 779. ISBN 9781133709510.
- ^ Nelsen, O. E. (1953) Comparative embryology of the vertebrates Blakiston, page 31.
- ^ Hafez, E. S. E.; Hafez, B. (2013). Reproduction in Farm Animals. John Wiley & Sons. ISBN 978-1-118-71028-9.
- ^ Vogelnest, Larry; Portas, Timothy (2019-05-01). Current Therapy in Medicine of Australian Mammals. Csiro Publishing. ISBN 978-1-4863-0753-1.
- ^ Society, Australian Mammal (December 1978). Australian Mammal Society. Australian Mammal Society.
- ^ Chenoweth, Peter J.; Lorton, Steven (2014). Animal Andrology: Theories and Applications. CABI. ISBN 978-1-78064-316-8.
- ^ C. Hugh Tyndale-Biscoe (2005). Life of Marsupials. Csiro Publishing. ISBN 978-0-643-06257-3.
- ^ John W. Hermanson; Howard E. Evans; Alexander de Lahunta (20 December 2018). Miller and Evans’ Anatomy of the Dog – E-Book. Elsevier Health Sciences. ISBN 978-0-323-54602-7.
- ^ Glover, Tim (2012-07-12). Mating Males: An Evolutionary Perspective on Mammalian Reproduction. p. 31. ISBN 9781107000018.
- ^ Ettinger, Stephen J.; Feldman, Edward C. (24 December 2009). Textbook of veterinary internal medicine : diseases of the dog and the cat (7th ed.). St. Louis, Mo. p. 2057. ISBN 9781437702828.
- ^ William F. Perrin; Bernd Würsig; J.G.M. Thewissen (26 February 2009). Encyclopedia of Marine Mammals. Academic Press. ISBN 978-0-08-091993-5.
- ^ Rommel, Sentiel A., D. Ann Pabst, and William A. McLellan. «Functional anatomy of the cetacean reproductive system, with comparisons to the domestic dog.» Reproductive Biology and Phylogeny of Cetacea. Science Publishers (2016): 127–145.
- ^ Coyne, Jerry A. (2009). Why Evolution is True. p. 90. ISBN 9780199230846.
- ^ Alan J., Wein; Louis R., Kavoussi; Alan W., Partin; Craig A., Peters (23 October 2015). Campbell-Walsh Urology (Eleventh ed.). Elsevier Health Sciences. pp. 1005–. ISBN 9780323263740.
- ^ Pastor Z, Chmel R (2017). «Differential diagnostics of female «sexual» fluids: a narrative review». International Urogynecology Journal. 29 (5): 621–629. doi:10.1007/s00192-017-3527-9. PMID 29285596. S2CID 5045626.
{{cite journal}}: CS1 maint: uses authors parameter (link) - ^ Bullough, Vern L.; Bullough, Bonnie (2014). Human Sexuality: An Encyclopedia. Routledge. p. 231. ISBN 978-1135825096.
- ^ Lentz, Gretchen M; Lobo, Rogerio A.; Gershenson, David M; Katz, Vern L. (2012). Comprehensive Gynecology. Elsevier Health Sciences, Philadelphia. p. 41. ISBN 978-0323091312.
- ^ Hornstein, Theresa; Schwerin, Jeri Lynn (2013). Biology of women. Clifton Park, NY: Delmar, Cengage Learning. p. 61. ISBN 978-1-285-40102-7. OCLC 911037670.
- ^ Toivanen R, Shen MM (2017). «Prostate organogenesis: tissue induction, hormonal regulation and cell type specification». Development. 144 (8): 1382–1398. doi:10.1242/dev.148270. PMC 5399670. PMID 28400434.
General and cited sources[edit]
- Ralston, Stuart H.; Penman, Ian D.; Strachan, Mark W.; Hobson, Richard P., eds. (2018). Davidson’s principles and practice of medicine (23rd ed.). Elsevier. ISBN 978-0-7020-7028-0.
- Attribution
- Portions of the text of this article originate from NIH Publication No. 02-4806, a public domain resource. «What I need to know about Prostate Problems». National Institutes of Health. 2002-06-01. No. 02-4806. Archived from the original on 2002-06-01. Retrieved 2011-01-24.
External links[edit]
 Media related to Prostate at Wikimedia Commons
Media related to Prostate at Wikimedia Commons
This article is about the male prostate gland. For the equivalent female prostate gland, see Skene’s gland. For the journal, see The Prostate.
| Prostate | |
|---|---|
|
|
| Details | |
| Precursor | Endodermic evaginations of the urethra |
| Artery | Internal pudendal artery, inferior vesical artery, and middle rectal artery |
| Vein | Prostatic venous plexus, pudendal plexus, vesical plexus, internal iliac vein |
| Nerve | Inferior hypogastric plexus |
| Lymph | internal iliac lymph nodes |
| Identifiers | |
| Latin | Prostata |
| MeSH | D011467 |
| TA98 | A09.3.08.001 |
| TA2 | 3637 |
| FMA | 9600 |
| Anatomical terminology
[edit on Wikidata] |
The prostate is both an accessory gland of the male reproductive system and a muscle-driven mechanical switch between urination and ejaculation. It is found in all male mammals.[1] It differs between species anatomically, chemically, and physiologically. Anatomically, the prostate is found below the bladder, with the urethra passing through it. It is described in gross anatomy as consisting of lobes and in microanatomy by zone. It is surrounded by an elastic, fibromuscular capsule and contains glandular tissue as well as connective tissue.
The prostate glands produce and contain fluid that forms part of semen, the substance emitted during ejaculation as part of the male sexual response. This prostatic fluid is slightly alkaline, milky or white in appearance. The alkalinity of semen helps neutralize the acidity of the vaginal tract, prolonging the lifespan of sperm. The prostatic fluid is expelled in the first part of ejaculate, together with most of the sperm, because of the action of smooth muscle tissue within the prostate. In comparison with the few spermatozoa expelled together with mainly seminal vesicular fluid, those in prostatic fluid have better motility, longer survival, and better protection of genetic material.
Disorders of the prostate include enlargement, inflammation, infection, and cancer. The word prostate comes from Ancient Greek προστάτης, prostátēs, meaning «one who stands before», «protector», «guardian», with the term originally used to describe the seminal vesicles.
Structure[edit]
The prostate is a gland of the male reproductive system. In adults, it is about the size of a walnut,[2] and has an average weight of about 11 grams, usually ranging between 7 and 16 grams.[3] The prostate is located in the pelvis. It sits below the urinary bladder and surrounds the urethra. The part of the urethra passing through it is called the prostatic urethra, which joins with the two ejaculatory ducts.[2] The prostate is covered in a surface called the prostatic capsule or prostatic fascia.[4]
The internal structure of the prostate has been described using both lobes and zones.[5][2] Because of the variation in descriptions and definitions of lobes, the zone classification is used more predominantly.[2]
The prostate has been described as consisting of three or four zones.[2][4] Zones are more typically able to be seen on histology, or in medical imaging, such as ultrasound or MRI.[2][5] The zones are:
| Name | Fraction of adult gland[2] | Description |
| Peripheral zone (PZ) | 70% | The back of the gland that surrounds the distal urethra and lies beneath the capsule. About 70–80% of prostatic cancers originate from this zone of the gland.[6][7] |
| Central zone (CZ) | 20% | This zone surrounds the ejaculatory ducts.[2] The central zone accounts for roughly 2.5% of prostate cancers; these cancers tend to be more aggressive and more likely to invade the seminal vesicles.[8] |
| Transition zone (TZ) | 5% | The transition zone surrounds the proximal urethra.[2] ~10–20% of prostate cancers originate in this zone. It is the region of the prostate gland that grows throughout life and causes the disease of benign prostatic enlargement.[6][7] |
| Anterior fibro-muscular zone (or stroma) | N/A | This area, not always considered a zone,[4] is usually devoid of glandular components and composed only, as its name suggests, of muscle and fibrous tissue.[2] |
The «lobe» classification describes lobes that, while originally defined in the fetus, are also visible in gross anatomy, including dissection and when viewed endoscopically.[5][4] The five lobes are the anterior lobe or isthmus, the posterior lobe, the right and left lateral lobes, and the middle or median lobe.
-
Lobes of prostate
-
Zones of prostate
Inside of the prostate, adjacent and parallel to the prostatic urethra, there are two longitudinal muscle systems. On the front side (ventrally) runs the urethral dilator (musculus dilatator urethrae), on the backside (dorsally) runs the muscle switching the urethra into the ejaculatory state (musculus ejaculatorius).[9]
Blood and lymphatic vessels[edit]
The prostate receives blood through the inferior vesical artery, internal pudendal artery, and middle rectal arteries. These vessels enter the prostate on its outer posterior surface where it meets the bladder, and travel forward to the apex of the prostate.[4] Both the inferior vesical and the middle rectal arteries often arise together directly from the internal iliac arteries. On entering the bladder, the inferior vesical artery splits into a urethral branch, supplying the urethral prostate; and a capsular branch, which travels around the capsule and has smaller branches which perforate into the prostate.[4]
The veins of the prostate form a network – the prostatic venous plexus, primarily around its front and outer surface.[4] This network also receives blood from the deep dorsal vein of the penis, and is connected via branches to the vesical plexus and internal pudendal veins.[4] Veins drain into the vesical and then internal iliac veins.[4]
The lymphatic drainage of the prostate depends on the positioning of the area. Vessels surrounding the vas deferens, some of the vessels in the seminal vesicle, and a vessel from the posterior surface of the prostate drain into the external iliac lymph nodes.[4] Some of the seminal vesicle vessels, prostatic vessels, and vessels from the anterior prostate drain into internal iliac lymph nodes.[4] Vessels of the prostate itself also drain into the obturator and sacral lymph nodes.[4]
Microanatomy[edit]
The prostate consists of glandular and connective tissue.[2] Tall column-shaped cells form the lining (the epithelium) of the glands.[2] These form one layer or may be pseudostratified.[4] The epithelium is highly variable and areas of low cuboidal or flat cells can also be present, with transitional epithelium in the outer regions of the longer ducts.[10] The glands are formed as many follicles, which in drain into canals and subsequently 12–20 main ducts, These in turn drain into the urethra as it passes through the prostate.[4] There are also a small amount of flat cells, which sit next to the basement membranes of glands, and act as stem cells.[2]
The connective tissue of the prostate is made up of fibrous tissue and smooth muscle.[2] The fibrous tissue separates the gland into lobules.[2] It also sits between the glands and is composed of randomly orientated smooth-muscle bundles that are continuous with the bladder.[11]
Over time, thickened secretions called corpora amylacea accumulate in the gland.[2]
-
Microscopic glands of the prostate
Gene and protein expression[edit]
About 20,000 protein coding genes are expressed in human cells and almost 75% of these genes are expressed in the normal prostate.[12][13] About 150 of these genes are more specifically expressed in the prostate, with about 20 genes being highly prostate specific.[14] The corresponding specific proteins are expressed in the glandular and secretory cells of the prostatic gland and have functions that are important for the characteristics of semen, including prostate-specific proteins, such as the prostate specific antigen (PSA), and the Prostatic acid phosphatase.[15]
Development[edit]
In the developing embryo, at the hind end lies an inpouching called the cloaca. This, over the fourth to the seventh week, divides into a urogenital sinus and the beginnings of the anal canal, with a wall forming between these two inpouchings called the urorectal septum.[16] The urogenital sinus divides into three parts, with the middle part forming the urethra; the upper part is largest and becomes the urinary bladder, and the lower part then changes depending on the biological sex of the embryo.[16]
The prostatic part of the urethra develops from the middle, pelvic, part of the urogenital sinus, which is of endodermal origin.[17] Around the end of the third month of embryonic life, outgrowths arise from the prostatic part of the urethra and grow into the surrounding mesenchyme.[17] The cells lining this part of the urethra differentiate into the glandular epithelium of the prostate.[17] The associated mesenchyme differentiates into the dense connective tissue and the smooth muscle of the prostate.[18]
Condensation of mesenchyme, urethra, and Wolffian ducts gives rise to the adult prostate gland, a composite organ made up of several tightly fused glandular and non-glandular components. To function properly, the prostate needs male hormones (androgens), which are responsible for male sex characteristics. The main male hormone is testosterone, which is produced mainly by the testicles. It is dihydrotestosterone (DHT), a metabolite of testosterone, that predominantly regulates the prostate. The prostate gland enlarges over time, until the fourth decade of life.[4]
Function[edit]
The prostate secretes fluid which becomes part of semen. Semen is the fluid emitted (ejaculated) by males during the sexual response.[19] When sperm is emitted, it is transmitted from the vas deferens into the male urethra via the ejaculatory ducts, which lie within the prostate gland.[19] Ejaculation is the expulsion of semen from the urethra.[19] Semen is moved into the urethra following contractions of the smooth muscle of the vas deferens and seminal vesicles, following stimulation, primarily of the glans penis. Stimulation sends nerve signals via the internal pudendal nerves to the upper lumbar spine; the nerve signals causing contraction act via the hypogastric nerves.[19] After traveling into the urethra, the seminal fluid is ejaculated by contraction of the bulbocavernosus muscle.[19] The secretions of the prostate include proteolytic enzymes, prostatic acid phosphatase, fibrinolysin, zinc, and prostate-specific antigen.[4] Together with the secretions from the seminal vesicles, these form the major fluid part of semen.[4]
It is possible for some men to achieve orgasm solely through stimulation of the prostate gland, such as via prostate massage or anal intercourse.[20][21] This has led to the area of the rectal wall adjacent to the prostate to be popularly referred by the anatomically incorrect term, the «male G-spot».[22]
The prostate’s changes of shape, which facilitate the mechanical switch between urination and ejaculation, are mainly driven by the two longitudinal muscle systems running along the prostatic urethra. These are the urethral dilator (musculus dilatator urethrae) on the urethra’s front side, which contracts during urination and thereby shortens and tilts the prostate in its vertical dimension thus widening the prostatic section of the urethral tube,[23][24] and the muscle switching the urethra into the ejaculatory state (musculus ejaculatorius) on its backside.[9]
In case of an operation, e.g. because of benign prostatic hyperplasia (BPH), damaging or sparing of these two muscle systems varies considerably depending on the choice of operation type and details of the procedure of the chosen technique. The effects on postoperational urination and ejaculation vary correspondingly.[25] (See also: Surgery for benign prostatic hyperplasia).
Clinical significance[edit]
Inflammation[edit]
Micrograph showing an inflamed prostate gland, found in prostatitis. A large amount of darker cells, representing leukocytes, can be seen. An area without inflammation is seen on the left of the image. H&E stain.
Prostatitis is inflammation of the prostate gland. It can be caused by infection with bacteria, or other noninfective causes. Inflammation of the prostate can cause painful urination or ejaculation, groin pain, difficulty passing urine, or constitutional symptoms such as fever or tiredness.[26] When inflamed, the prostate becomes enlarged and is tender when touched during digital rectal examination. The bacteria responsible for the infection may be detected by a urine culture.[26]
Acute prostatitis and chronic bacterial prostatitis are treated with antibiotics.[26] Chronic non-bacterial prostatitis, or male chronic pelvic pain syndrome is treated by a large variety of modalities including the medications alpha blockers, nonsteroidal antiinflammatories and amitriptyline,[26] antihistamines, and other anxiolytics.[27] Other treatments that are not medications may include physical therapy,[28] psychotherapy, nerve modulators, and surgery. More recently, a combination of trigger point and psychological therapy has proved effective for category III prostatitis as well.[27]
Enlarged prostate[edit]
A diagram of prostate cancer pressing on the urethra, which can cause symptoms
An enlarged prostate is called prostatomegaly, with benign prostatic hyperplasia (BPH) being the most common cause. BPH refers to an enlargement of the prostate due to an increase in the number of cells that make up the prostate (hyperplasia) from a cause that is not a malignancy. It is very common in older men.[26] It is often diagnosed when the prostate has enlarged to the point where urination becomes difficult. Symptoms include needing to urinate often (urinary frequency) or taking a while to get started (urinary hesitancy). If the prostate grows too large, it may constrict the urethra and impede the flow of urine, making urination painful and difficult, or in extreme cases completely impossible, causing urinary retention.[26] Over time, chronic retention may cause the bladder to become larger and cause a backflow of urine into the kidneys (hydronephrosis).[26]
BPH can be treated with medication, a minimally invasive procedure or, in extreme cases, surgery that removes the prostate. In general, treatment often begins with an alpha-1 adrenergic receptor antagonist medication such as tamsulosin, which reduces the tone of the smooth muscle found in the urethra that passes through the prostate, making it easier for urine to pass through.[26] For people with persistent symptoms, procedures may be considered. The surgery most often used in such cases is transurethral resection of the prostate,[26] in which an instrument is inserted through the urethra to remove prostate tissue that is pressing against the upper part of the urethra and restricting the flow of urine. Minimally invasive procedures include transurethral needle ablation of the prostate and transurethral microwave thermotherapy.[29] These outpatient procedures may be followed by the insertion of a temporary stent, to allow normal voluntary urination, without exacerbating irritative symptoms.[30]
Cancer[edit]
Prostate cancer is one of the most common cancers affecting older men in the UK, US, Northern Europe and Australia, and a significant cause of death for elderly men worldwide.[31] Often, a person does not have symptoms; when they do occur, symptoms may include urinary frequency, urgency, hesitation and other symptoms associated with BPH. Uncommonly, such cancers may cause weight loss, retention of urine, or symptoms such as back pain due to metastatic lesions that have spread outside of the prostate.[26]
A digital rectal examination and the measurement of a prostate-specific antigen (PSA) level are usually the first investigations done to check for prostate cancer. PSA values are difficult to interpret, because a high value might be present in a person without cancer, and a low value can be present in someone with cancer.[26] The next form of testing is often the taking of a biopsy to assess for tumour activity and invasiveness.[26] Because of the significant risk of overdiagnosis with widespread screening in the general population, prostate cancer screening is controversial.[32] If a tumour is confirmed, medical imaging such as an MRI or bone scan may be done to check for the presence of tumour metastases in other parts of the body.[26]
Prostate cancer that is only present in the prostate is often treated with either surgical removal of the prostate or with radiotherapy or by the insertion of small radioactive particles of iodine-125 or palladium-103, called brachytherapy.[33][26] Cancer that has spread to other parts of the body is usually treated also with hormone therapy, to deprive a tumour of sex hormones (androgens) that stimulate proliferation. This is often done through the use of GnRH analogues or agents (such as bicalutamide) that block the receptors that androgens act on; occasionally, surgical removal of the testes may be done instead.[26] Cancer that does not respond to hormonal treatment, or that progresses after treatment, might be treated with chemotherapy such as docetaxel. Radiotherapy may also be used to help with pain associated with bony lesions.[26]
Sometimes, the decision may be made not to treat prostate cancer. If a cancer is small and localised, the decision may be made to monitor for cancer activity at intervals («active surveillance») and defer treatment.[26] If a person, because of frailty or other medical conditions or reasons, has a life expectancy less than ten years, then the impacts of treatment may outweigh any perceived benefits.[26]
Surgery[edit]
Surgery to remove the prostate is called prostatectomy, and is usually done as a treatment for cancer limited to the prostate, or prostatic enlargement.[34] When it is done, it may be done as open surgery or as laparoscopic (keyhole) surgery.[34] These are done under general anaesthetic.[35] Usually the procedure for cancer is a radical prostatectomy, which means that the seminal vesicles are removed and vas deferens is also tied off.[34] Part of the prostate can also be removed from within the urethra, called transurethral resection of the prostate (TURP).[34] Open surgery may involve a cut that is made in the perineum, or via an approach that involves a cut down the midline from the belly button to the pubic bone.[34] Open surgery may be preferred if there is a suspicion that lymph nodes are involved and they need to be removed or biopsied during a procedure.[34] A perineal approach will not involve lymph node removal and may result in less pain and a faster recovery following an operation.[34] A TURP procedure uses a tube inserted into the urethra via the penis and some form of heat, electricity or laser to remove prostate tissue.[34]
The whole prostate can be removed. Complications that might develop because of surgery include urinary incontinence and erectile dysfunction because of damage to nerves during the operation, particularly if a cancer is very close to nerves.[34][35] Ejaculation of semen will not occur during orgasm if the vas deferens are tied off and seminal vesicles removed, such as during a radical prosatectomy.[34] This will mean a man becomes infertile.[34] Sometimes, orgasm may not be able to occur or may be painful. The penis length may change if the part of the urethra within the prostate is also removed.[34] General complications due to surgery can also develop, such as infections, bleeding, inadvertent damage to nearby organs or within the abdomen, and the formation of blood clots.[34]
History[edit]
The prostate was first formally identified by Venetian anatomist Niccolò Massa in Anatomiae libri introductorius (Introduction to Anatomy) 1536 and illustrated by Flemish anatomist Andreas Vesalius in Tabulae anatomicae sex (six anatomical tables) in 1538.[36][5] Massa described it as a «glandular flesh upon which rests the neck of the bladder,» and Vesalius as a «glandular body».[37] The first time a word similar to ‘prostate’ was used to describe the gland is credited to André du Laurens in 1600, who described it as a term already in use by anatomists at the time.[37][5] The term was however used at least as early as 1549 by French surgeon Ambroise Pare.[5]
At the time, Du Laurens was describing what was considered to be a pair of organs (not the single two-lobed organ), and the Latin term prostatae that was used was a mistranslation of the term for the Ancient Greek word used to describe the seminal vesicles, parastatai;[37] although it has been argued that surgeons in Ancient Greece and Rome must have at least seen the prostate as an anatomical entity.[5] The term prostatae was taken rather than the grammatically correct prostator (singular) and prostatores (plural) because the gender of the Ancient Greek term was taken as female, when it was in fact male.[37]
The fact that the prostate was one and not two organs was an idea popularised throughout the early 18th century, as was the English language term used to describe the organ, prostate,[37] attributed to William Cheselden.[38] A monograph, «Practical observations on the treatment of the diseases of the prostate gland» by Everard Home in 1811, was important in the history of the prostate by describing and naming anatomical parts of the prostate, including the median lobe.[37] The idea of the five lobes of the prostate was popularized following anatomical studies conducted by American urologist Oswald Lowsley in 1912.[5][38] John E. McNeal first proposed the idea of «zones» in 1968; McNeal found that the relatively homogeneous cut surface of an adult prostate in no way resembled «lobes» and thus led to the description of «zones».[39]
Prostate cancer was first described in a speech to the Medical and Chiurgical Society of London in 1853 by surgeon John Adams[40][41] and increasingly described by the late 19th century.[42] Prostate cancer was initially considered a rare disease, probably because of shorter life expectancies and poorer detection methods in the 19th century. The first treatments of prostate cancer were surgeries to relieve urinary obstruction.[43] Samuel David Gross has been credited with the first mention of a prostatectomy, as «too absurd to be seriously entertained»[44][42] The first removal for prostate cancer (radical perineal prostatectomy) was first performed in 1904 by Hugh H. Young at Johns Hopkins Hospital;[45][42] partial removal of the gland was conducted by Theodore Billroth in 1867.[38]
Transurethral resection of the prostate (TURP) replaced radical prostatectomy for symptomatic relief of obstruction in the middle of the 20th century because it could better preserve penile erectile function. Radical retropubic prostatectomy was developed in 1983 by Patrick Walsh.[46] In 1941, Charles B. Huggins published studies in which he used estrogen to oppose testosterone production in men with metastatic prostate cancer. This discovery of «chemical castration» won Huggins the 1966 Nobel Prize in Physiology or Medicine.[47]
The role of the gonadotropin-releasing hormone (GnRH) in reproduction was determined by Andrzej W. Schally and Roger Guillemin, who both won the 1977 Nobel Prize in Physiology or Medicine for this work. GnRH receptor agonists, such as leuprorelin and goserelin, were subsequently developed and used to treat prostate cancer.[48][49] Radiation therapy for prostate cancer was first developed in the early 20th century and initially consisted of intraprostatic radium implants. External beam radiotherapy became more popular as stronger X-ray radiation sources became available in the middle of the 20th century. Brachytherapy with implanted seeds (for prostate cancer) was first described in 1983.[50] Systemic chemotherapy for prostate cancer was first studied in the 1970s. The initial regimen of cyclophosphamide and 5-fluorouracil was quickly joined by multiple regimens using a host of other systemic chemotherapy drugs.[51]
Other animals[edit]
The prostate is found only in mammals.[52] The prostate glands of male marsupials are proportionally larger than those of placental mammals.[53] The presence of a functional prostate in monotremes is controversial, and if monotremes do possess functional prostates, they may not make the same contribution to semen as in other mammals.[54]
The structure of the prostate varies, ranging from tubuloalveolar (as in humans) to branched tubular. The gland is particularly well developed in dogs, foxes and boars, though in other mammals, such as bulls, it can be small and inconspicuous.[55][56][57] In other animals, such as marsupials[58][59] and small ruminants, the prostate is disseminate, meaning not specifically localisable as a distinct tissue, but present throughout the relevant part of the urethra; in other animals, such as red deer and American elk, it may be present as a specific organ and in a disseminate form.[60] In some marsupial species, the size of the prostate gland changes seasonally.[61] The prostate is the only accessory gland that occurs in male dogs.[62] Dogs can produce in one hour as much prostatic fluid as a human can in a day. They excrete this fluid along with their urine to mark their territory.[63] Additionally, dogs are the only species apart from humans seen to have a significant incidence of prostate cancer.[64] In cetaceans (whales, dolphins, porpoises) the prostate is composed of diffuse urethral glands[65] and is surrounded by a very powerful compressor muscle.[66]
The prostate gland originates with tissues in the urethral wall.[citation needed] This means the urethra, a compressible tube used for urination, runs through the middle of the prostate. This leads to an evolutionary design fault for some mammals, including human males. The prostate is prone to infection and enlargement later in life, constricting the urethra so urinating becomes slow and painful.[67]
Prostatic secretions vary among species. They are generally composed of simple sugars and are often slightly alkaline.[68]
Skene’s gland[edit]
Because the Skene’s gland and the male prostate act similarly by secreting prostate-specific antigen (PSA), which is an ejaculate protein produced in males, and of prostate-specific acid phosphatase, the Skene’s gland is sometimes referred to as the «female prostate».[69][70] Although it is homologous to the male prostate (developed from the same embryological tissues),[71][72] various aspects of its development in relation to the male prostate are widely unknown and a matter of research.[73]
See also[edit]
- Ejaculatory duct
- Seminal vesicles
- Prostate evolution in monotreme mammals
References[edit]
Citations[edit]
- ^ Vásquez, Bélgica (2014-03-01). «Morphological Characteristics of Prostate in Mammals». International Journal of Medical and Surgical Sciences. 1 (1): 63–72. doi:10.32457/ijmss.2014.010. ISSN 0719-532X.
- ^ a b c d e f g h i j k l m n o p Young, Barbara; O’Dowd, Geraldine; Woodford, Phillip (2013). Wheater’s functional histology: a text and colour atlas (6th ed.). Philadelphia: Elsevier. pp. 347–8. ISBN 9780702047473.
- ^ Leissner KH, Tisell LE (1979). «The weight of the human prostate». Scand. J. Urol. Nephrol. 13 (2): 137–42. doi:10.3109/00365597909181168. PMID 90380.
- ^ a b c d e f g h i j k l m n o p q Standring, Susan, ed. (2016). «Prostate». Gray’s anatomy : the anatomical basis of clinical practice (41st ed.). Philadelphia. pp. 1266–1270. ISBN 9780702052309. OCLC 920806541.
- ^ a b c d e f g h Goddard, Jonathan Charles (January 2019). «The history of the prostate, part one: say what you see». Trends in Urology & Men’s Health. 10 (1): 28–30. doi:10.1002/tre.676.
- ^ a b «Basic Principles: Prostate Anatomy» Archived 2010-10-15 at the Wayback Machine. Urology Match. Www.urologymatch.com. Web. 14 June 2010.
- ^ a b «Prostate Cancer Information from the Foundation of the Prostate Gland.» Prostate Cancer Treatment Guide. Web. 14 June 2010.
- ^ Cohen RJ, Shannon BA, Phillips M, Moorin RE, Wheeler TM, Garrett KL (2008). «Central zone carcinoma of the prostate gland: a distinct tumor type with poor prognostic features». The Journal of Urology. 179 (5): 1762–7, discussion 1767. doi:10.1016/j.juro.2008.01.017. PMID 18343454.
- ^ a b Michael Schünke, Erik Schulte, Udo Schumacher: PROMETHEUS Innere Organe. LernAtlas Anatomie, vol 2: Innere Organe, Thieme Verlag, Stuttgart/Germany 2012, ISBN 9783131395337, p. 298, PDF.
- ^ «Prostate Gland Development». ana.ed.ac.uk. Archived from the original on 2003-04-30. Retrieved 2011-08-03.
- ^ «Prostate». webpath.med.utah.edu. Retrieved 2019-11-17.
- ^ «The human proteome in prostate – The Human Protein Atlas». www.proteinatlas.org. Retrieved 2017-09-26.
- ^ Uhlén, Mathias; Fagerberg, Linn; Hallström, Björn M.; Lindskog, Cecilia; Oksvold, Per; Mardinoglu, Adil; Sivertsson, Åsa; Kampf, Caroline; Sjöstedt, Evelina (2015-01-23). «Tissue-based map of the human proteome». Science. 347 (6220): 1260419. doi:10.1126/science.1260419. ISSN 0036-8075. PMID 25613900. S2CID 802377.
- ^ O’Hurley, Gillian; Busch, Christer; Fagerberg, Linn; Hallström, Björn M.; Stadler, Charlotte; Tolf, Anna; Lundberg, Emma; Schwenk, Jochen M.; Jirström, Karin (2015-08-03). «Analysis of the Human Prostate-Specific Proteome Defined by Transcriptomics and Antibody-Based Profiling Identifies TMEM79 and ACOXL as Two Putative, Diagnostic Markers in Prostate Cancer». PLOS ONE. 10 (8): e0133449. Bibcode:2015PLoSO..1033449O. doi:10.1371/journal.pone.0133449. ISSN 1932-6203. PMC 4523174. PMID 26237329.
- ^ Kong, HY; Byun, J (January 2013). «Emerging roles of human prostatic Acid phosphatase». Biomolecules & Therapeutics. 21 (1): 10–20. doi:10.4062/biomolther.2012.095. PMC 3762301. PMID 24009853.
- ^ a b Sadley, TW (2019). «Bladder and urethra». Langman’s medical embryology (14th ed.). Philadelphia: Wolters Kluwer. pp. 263–66. ISBN 9781496383907.
- ^ a b c Sadley, TW (2019). Langman’s medical embryology (14th ed.). Philadelphia: Wolters Kluwer. pp. 265–6. ISBN 9781496383907.
- ^ Moore, Keith L.; Persaud, T. V. N.; Torchia, Mark G. (2008). Before We are Born: Essentials of Embryology and Birth Defects (7th ed.). ISBN 978-1-4160-3705-7.
- ^ a b c d e Barrett, Kim E. (2019). Ganong’s review of medical physiology. Barman, Susan M.,, Brooks, Heddwen L.,, Yuan, Jason X.-J. (26th ed.). New York. pp. 411, 415. ISBN 9781260122404. OCLC 1076268769.
- ^ Rosenthal, Martha (2012). Human Sexuality: From Cells to Society. Cengage Learning. pp. 133–135. ISBN 978-0618755714. Retrieved September 17, 2012.
- ^ Komisaruk, Barry R.; Whipple, Beverly; Nasserzadeh, Sara & Beyer-Flores, Carlos (2009). The Orgasm Answer Guide. JHU Press. pp. 108–109. ISBN 978-0-8018-9396-4. Retrieved 6 November 2011.
- ^ Levin, R. J. (2018). «Prostate-induced orgasms: A concise review illustrated with a highly relevant case study». Clinical Anatomy. 31 (1): 81–85. doi:10.1002/ca.23006. PMID 29265651.
- ^ Hocaoglu Y, Roosen A, Herrmann K, Tritschler S, Stief C, Bauer RM (2012). «Real-time magnetic resonance imaging (MRI): anatomical changes during physiological voiding in men». BJU Int. 109 (2): 234–9. doi:10.1111/j.1464-410X.2011.10255.x. PMID 21736694.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ^ Hocaoglu Y, Herrmann K, Walther S, Hennenberg M, Gratzke C, Bauer R; et al. (2013). «Contraction of the anterior prostate is required for the initiation of micturition». BJU Int. 111 (7): 1117–23. doi:10.1111/j.1464-410X.2012.11698.x. PMID 23356864.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ^ Lebdai S, Chevrot A, Doizi S, Pradere B, Delongchamps NB, Benchikh A; et al. (2019). «Do patients have to choose between ejaculation and miction? A systematic review about ejaculation preservation technics for benign prostatic obstruction surgical treatment» (PDF). World J Urol. 37 (2): 299–308. doi:10.1007/s00345-018-2368-6. PMID 29967947. S2CID 49556196. Archived from the original (PDF) on 2021-08-11. Retrieved 2020-11-16.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ^ a b c d e f g h i j k l m n o p q r Davidson’s 2018, pp. 437–9.
- ^ a b Anderson RU, Wise D, Sawyer T, Chan CA (2006). «Sexual dysfunction in men with chronic prostatitis/chronic pelvic pain syndrome: improvement after trigger point release and paradoxical relaxation training». J. Urol. 176 (4 Pt 1): 1534–8, discussion 1538–9. CiteSeerX 10.1.1.383.7495. doi:10.1016/j.juro.2006.06.010. PMID 16952676.
- ^ «Physical Therapy Treatment for Prostatitis/chronic pelvic pain syndrome». 2014. Retrieved 2014-10-22.
- ^ Christensen, TL; Andriole, GL (February 2009). «Benign Prostatic Hyperplasia: Current Treatment Strategies». Consultant. 49 (2).
- ^ Dineen MK, Shore ND, Lumerman JH, Saslawsky MJ, Corica AP (2008). «Use of a Temporary Prostatic Stent After Transurethral Microwave Thermotherapy Reduced Voiding Symptoms and Bother Without Exacerbating Irritative Symptoms». J. Urol. 71 (5): 873–877. doi:10.1016/j.urology.2007.12.015. PMID 18374395.
- ^ Rawla P (April 2019). «Epidemiology of Prostate Cancer». World J Oncol (Review). 10 (2): 63–89. doi:10.14740/wjon1191. PMC 6497009. PMID 31068988.
- ^ Sandhu, Gurdarshan S.; Andriole, Gerald L. (September 2012). «Overdiagnosis of Prostate Cancer». Journal of the National Cancer Institute. Monographs. 2012 (45): 146–151. doi:10.1093/jncimonographs/lgs031. ISSN 1052-6773. PMC 3540879. PMID 23271765.
- ^ «What is Brachytherapy?». American Brachytherapy Society. Retrieved 8 August 2020.
- ^ a b c d e f g h i j k l m «Surgery for Prostate Cancer». www.cancer.org. The American Cancer Society medical and editorial content team. 1 August 2019. Retrieved 8 August 2020.
- ^ a b «Surgery to remove your prostate gland | Prostate cancer | Cancer Research UK». www.cancerresearchuk.org. Cancer Research UK. 18 Jun 2019. Retrieved 8 August 2020.
- ^ Ghabili, Kamyar; Tosoian, Jeffrey J.; Schaeffer, Edward M.; Pavlovich, Christian P.; Golzari, Samad E.J.; Khajir, Ghazal; Andreas, Darian; Benzon, Benjamin; Vuica-Ross, Milena; Ross, Ashley E. (November 2016). «The History of Prostate Cancer From Antiquity: Review of Paleopathological Studies». Urology. 97: 8–12. doi:10.1016/j.urology.2016.08.032. PMID 27591810.
- ^ a b c d e f Josef Marx, Franz; Karenberg, Axel (1 February 2009). «History of the Term Prostate». The Prostate. 69 (2): 208–213. doi:10.1002/pros.20871. PMID 18942121. S2CID 44922919.
- ^ a b c Young, Robert H; Eble, John N (January 2019). «The history of urologic pathology: an overview». Histopathology. 74 (1): 184–212. doi:10.1111/his.13753. PMID 30565309. S2CID 56476748.
- ^ Myers, Robert P (2000). «Structure of the adult prostate from a clinician’s standpoint». Clinical Anatomy. 13 (3): 214–5. doi:10.1002/(SICI)1098-2353(2000)13:3<214::AID-CA10>3.0.CO;2-N. PMID 10797630. S2CID 33861863.
- ^ Adams J (1853). «The case of scirrhous of the prostate gland with corresponding affliction of the lymphatic glands in the lumbar region and in the pelvis». Lancet. 1 (1547): 393–94. doi:10.1016/S0140-6736(02)68759-8.
- ^ Ghabili K, Tosoian JJ, Schaeffer EM, Pavlovich CP, Golzari SE, Khajir G, Andreas D, Benzon B, Vuica-Ross M, Ross AE (November 2016). «The History of Prostate Cancer From Antiquity: Review of Paleopathological Studies». Urology. 97: 8–12. doi:10.1016/j.urology.2016.08.032. PMID 27591810.
- ^ a b c Nahon, I; Waddington, G; Dorey, G; Adams, R (2011). «The history of urologic surgery: from reeds to robotics». Urologic Nursing. 31 (3): 173–80. doi:10.7257/1053-816X.2011.31.3.173. PMID 21805756.
- ^ Lytton B (June 2001). «Prostate cancer: a brief history and the discovery of hormonal ablation treatment». The Journal of Urology. 165 (6 Pt 1): 1859–62. doi:10.1016/S0022-5347(05)66228-3. PMID 11371867.
- ^ Samuel David Gross (1851). A Practical Treatise On the Diseases and Injuries of the Urinary Bladder, the Prostate Gland, and the Urethra. Philadelphia: Blanchard and Lea.
«The idea of extirpating the entire gland is, indeed, too absurd to be seriously entertained… Excision of the middle lobe would be far less objectionable»
- ^ Young HH (1905). «Four cases of radical prostatectomy». Johns Hopkins Bull. 16.
- ^ Walsh PC, Lepor H, Eggleston JC (1983). «Radical prostatectomy with preservation of sexual function: anatomical and pathological considerations». The Prostate. 4 (5): 473–85. doi:10.1002/pros.2990040506. PMID 6889192. S2CID 30740301.
- ^ Huggins CB, Hodges CV (1941). «Studies on prostate cancer: 1. The effects of castration, of estrogen and androgen injection on serum phosphatases in metastatic carcinoma of the prostate». Cancer Res. 1 (4): 293. Archived from the original on 2017-06-30.
- ^ Schally AV, Kastin AJ, Arimura A (November 1971). «Hypothalamic follicle-stimulating hormone (FSH) and luteinizing hormone (LH)-regulating hormone: structure, physiology, and clinical studies». Fertility and Sterility. 22 (11): 703–21. doi:10.1016/S0015-0282(16)38580-6. PMID 4941683.
- ^ Tolis G, Ackman D, Stellos A, Mehta A, Labrie F, Fazekas AT, et al. (March 1982). «Tumor growth inhibition in patients with prostatic carcinoma treated with luteinizing hormone-releasing hormone agonists». Proceedings of the National Academy of Sciences of the United States of America. 79 (5): 1658–62. Bibcode:1982PNAS…79.1658T. doi:10.1073/pnas.79.5.1658. PMC 346035. PMID 6461861.
- ^ Denmeade SR, Isaacs JT (May 2002). «A history of prostate cancer treatment». Nature Reviews. Cancer. 2 (5): 389–96. doi:10.1038/nrc801. PMC 4124639. PMID 12044015.
- ^ Scott WW, Johnson DE, Schmidt JE, Gibbons RP, Prout GR, Joiner JR, et al. (December 1975). «Chemotherapy of advanced prostatic carcinoma with cyclophosphamide or 5-fluorouracil: results of first national randomized study». The Journal of Urology. 114 (6): 909–11. doi:10.1016/S0022-5347(17)67172-6. PMID 1104900.
- ^ Marker, Paul C; Donjacour, Annemarie A; Dahiya, Rajvir; Cunha, Gerald R (January 2003). «Hormonal, cellular, and molecular control of prostatic development». Developmental Biology. 253 (2): 165–174. doi:10.1016/s0012-1606(02)00031-3. PMID 12645922.
- ^ Hugh Tyndale-Biscoe; Marilyn Renfree (30 January 1987). Reproductive Physiology of Marsupials. Cambridge University Press. ISBN 978-0-521-33792-2.
- ^ Temple-Smith, P; Grant, T (2001). «Uncertain breeding: a short history of reproduction in monotremes». Reproduction, Fertility, and Development. 13 (7–8): 487–97. doi:10.1071/rd01110. PMID 11999298.
- ^ Sherwood, Lauralee; Klandorf, Hillar; Yancey, Paul (January 2012). Animal Physiology: From Genes to Organisms. p. 779. ISBN 9781133709510.
- ^ Nelsen, O. E. (1953) Comparative embryology of the vertebrates Blakiston, page 31.
- ^ Hafez, E. S. E.; Hafez, B. (2013). Reproduction in Farm Animals. John Wiley & Sons. ISBN 978-1-118-71028-9.
- ^ Vogelnest, Larry; Portas, Timothy (2019-05-01). Current Therapy in Medicine of Australian Mammals. Csiro Publishing. ISBN 978-1-4863-0753-1.
- ^ Society, Australian Mammal (December 1978). Australian Mammal Society. Australian Mammal Society.
- ^ Chenoweth, Peter J.; Lorton, Steven (2014). Animal Andrology: Theories and Applications. CABI. ISBN 978-1-78064-316-8.
- ^ C. Hugh Tyndale-Biscoe (2005). Life of Marsupials. Csiro Publishing. ISBN 978-0-643-06257-3.
- ^ John W. Hermanson; Howard E. Evans; Alexander de Lahunta (20 December 2018). Miller and Evans’ Anatomy of the Dog – E-Book. Elsevier Health Sciences. ISBN 978-0-323-54602-7.
- ^ Glover, Tim (2012-07-12). Mating Males: An Evolutionary Perspective on Mammalian Reproduction. p. 31. ISBN 9781107000018.
- ^ Ettinger, Stephen J.; Feldman, Edward C. (24 December 2009). Textbook of veterinary internal medicine : diseases of the dog and the cat (7th ed.). St. Louis, Mo. p. 2057. ISBN 9781437702828.
- ^ William F. Perrin; Bernd Würsig; J.G.M. Thewissen (26 February 2009). Encyclopedia of Marine Mammals. Academic Press. ISBN 978-0-08-091993-5.
- ^ Rommel, Sentiel A., D. Ann Pabst, and William A. McLellan. «Functional anatomy of the cetacean reproductive system, with comparisons to the domestic dog.» Reproductive Biology and Phylogeny of Cetacea. Science Publishers (2016): 127–145.
- ^ Coyne, Jerry A. (2009). Why Evolution is True. p. 90. ISBN 9780199230846.
- ^ Alan J., Wein; Louis R., Kavoussi; Alan W., Partin; Craig A., Peters (23 October 2015). Campbell-Walsh Urology (Eleventh ed.). Elsevier Health Sciences. pp. 1005–. ISBN 9780323263740.
- ^ Pastor Z, Chmel R (2017). «Differential diagnostics of female «sexual» fluids: a narrative review». International Urogynecology Journal. 29 (5): 621–629. doi:10.1007/s00192-017-3527-9. PMID 29285596. S2CID 5045626.
{{cite journal}}: CS1 maint: uses authors parameter (link) - ^ Bullough, Vern L.; Bullough, Bonnie (2014). Human Sexuality: An Encyclopedia. Routledge. p. 231. ISBN 978-1135825096.
- ^ Lentz, Gretchen M; Lobo, Rogerio A.; Gershenson, David M; Katz, Vern L. (2012). Comprehensive Gynecology. Elsevier Health Sciences, Philadelphia. p. 41. ISBN 978-0323091312.
- ^ Hornstein, Theresa; Schwerin, Jeri Lynn (2013). Biology of women. Clifton Park, NY: Delmar, Cengage Learning. p. 61. ISBN 978-1-285-40102-7. OCLC 911037670.
- ^ Toivanen R, Shen MM (2017). «Prostate organogenesis: tissue induction, hormonal regulation and cell type specification». Development. 144 (8): 1382–1398. doi:10.1242/dev.148270. PMC 5399670. PMID 28400434.
General and cited sources[edit]
- Ralston, Stuart H.; Penman, Ian D.; Strachan, Mark W.; Hobson, Richard P., eds. (2018). Davidson’s principles and practice of medicine (23rd ed.). Elsevier. ISBN 978-0-7020-7028-0.
- Attribution
- Portions of the text of this article originate from NIH Publication No. 02-4806, a public domain resource. «What I need to know about Prostate Problems». National Institutes of Health. 2002-06-01. No. 02-4806. Archived from the original on 2002-06-01. Retrieved 2011-01-24.
External links[edit]
- Media related to Prostate at Wikimedia Commons
Роль предстательной железы в организме
Предстательная железа важна для сохранения мужской фертильности — способности к зачатию. Она выделяет секрет, являющийся компонентом спермы. Также состояние простаты влияет на эрекцию и мочеиспускание.
Предстательная железа закладывается на третьем месяце эмбрионального развития и начинает активно развиваться после шести лет. Окончательно формируется в период полового созревания и остается активной примерно до 45 лет. Позднее этого возраста начинается перерождение железистой ткани, орган постепенно перестает выполнять свои функции и атрофируется по мере снижения сексуальной активности.
В норме простата никак не проявляет себя и мужчина не чувствует ее работу или то, как она изменяется с возрастом. Если предстательная железа здорова, не должно быть боли, дискомфорта или ухудшения самочувствия, связанных с нею¹.
Когда нужно проходить профилактические осмотры у уролога?
Периодически всем мужчинам нужно посещать уролога — даже в случае, если их ничего не беспокоит. Профилактические осмотры проводятся в следующем возрасте:
- 12-14 лет;
- 20-35 лет — при появлении факторов риска (перенесенные половые инфекции, воспаления);
- старше 40-45 лет — профилактический осмотр проводится каждые три года для контроля риска аденомы и рака простаты.
Уролог может рекомендовать проходить осмотр чаще, если есть факторы риска возникновения заболеваний простаты.
Где расположена простата?
Знать, где находится простата, важно, чтобы вовремя распознать боли в ней, если они начнутся. Орган расположен в центре мужского таза под мочевым пузырем за лобковой костью (рис 1.). Железа опоясывает начальный отдел мочеиспускательного канала, шейку мочевого пузыря. Снизу ее поддерживают мышцы мочеполовой диафрагмы, а спереди — лобково-предстательные связки. У верхней задней части органа проходят семявыносящие протоки. Предстательная железа отделена от прямой кишки и прощупывается при пальпации через задний проход².
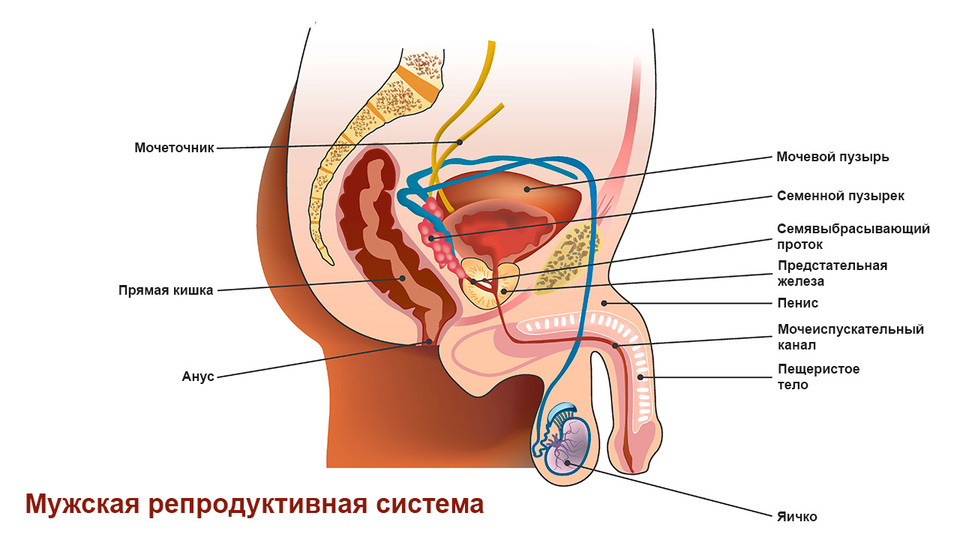
Строение простаты
Предстательная железа имеет форму ореха и состоит из пяти долей: правой и левой боковых, передней, задней, средней. У нее небольшие размеры — до 3 см в длину или ширину. В норме она весит около 20-25 г².
В строении простаты выделяют пять зон:
- Центральная — находится в основании железы, окружает правый и левый эякуляторные протоки.
- Переходная — располагается вокруг уретры, может увеличиваться в зрелом или пожилом возрасте.
- Периферическая — задняя и боковая стороны органа.
- Передний сегмент — часть, обращенная к лобковой кости.
- Зона сфинктера мочевого пузыря.
В центральной части простату разделяет канал уретры. Железа окружена большим количеством кровеносных сосудов, обеспечивающих ее кровоснабжение.
С возрастом строение простаты изменяется:
- До полового созревания она сформирована в основном мышечными тканями, а ее размер невелик.
- В период половой активности размеры железы увеличиваются и в основном она состоит из железистой ткани.
- По мере снижения половой активности в зрелом или пожилом возрасте в норме простата уменьшается в размерах, но также может происходить ее увеличение, и тогда нужно лечение у уролога.
Некоторые особенности рациона действительно могут влиять на риск заболеваний предстательной железы. В основном рекомендации по питанию направлены на профилактику аденомы простаты:
- Лучше пить меньше жидкости перед сном или перед выходом на улицу в холодную погоду.
- Кофе и спиртные напитки могут оказывать мочегонное действие, и лучше ограничить их употребление.
- В рацион лучше включать больше продуктов с низким содержанием жиров.
- Каждый день нужно есть свежие овощи и фрукты.
- Важно контролировать вес и не употреблять слишком калорийные продукты.
Для здоровья простаты полезны следующие продукты:
- томаты;
- ягоды;
- брокколи;
- орехи;
- нежирная рыба;
- цитрусовые;
- лук и чеснок;
- зеленый чай.
Вредными считаются молочные продукты с высокой жирностью, красное и жирное мясо, кофеин, алкоголь, а также продукты с высоким содержанием соли⁴.
Функции простаты
Простата выполняет три основные функции:
- Вырабатывает секрет для производства спермы.
- Перекрывает уретру при эякуляции.
- Участвует в гормональном обмене.
Секрет предстательной железы составляет около 1/3 от объема эякулята. Он нужен, чтобы сперматозоиды имели нормальную оплодотворяющую способность. В нем содержатся белковые вещества, ферменты, лейкоциты, эпителиальные клетки. Содержащиеся в секрете ферменты разжижают эякулят, облегчая движение сперматозоидов, и поэтому здоровье предстательной железы важно для сохранения фертильности.
Во время эякуляции простата сокращается и перекрывает уретру, делая невозможным опорожнение мочевого пузыря. Содержимое семенного пузырька смешивается с секретом предстательной железы и сперматозоидами и быстро проталкивается по мочеиспускательному каналу при эякуляции. Мочевой пузырь в это время перекрыт, поэтому нельзя одновременно эякулировать и мочиться.
Производящийся в простате фермент 5-альфа-редуктаза обеспечивает преобразование тестостерона в биологически более активную форму — дигидротестостерон. Это важно при развитии вторичных половых признаков у мужчин³.
Как болит простата?
Проблемы с простатой могут проявляться следующими симптомами:
- Боль, возникающая при эякуляции или мочеиспускании либо после них.
- Боль в мошонке, в области между мошонкой и анальным отверстием, в половом члене.
- Появление крови в моче, ее необычный запах или цвет.
- Дискомфорт, неприятные или болезненные ощущения в нижней части живота.
- Проблемы с мочеиспусканием: сложно начать мочиться, струя мочи слабая, в конце мочеиспускания есть подтекание, во время мочеиспускания происходят остановки или задержки, не удается полностью опорожнить мочевой пузырь.
- Позывы к мочеиспусканию возникают слишком часто, и их сложно контролировать.
- Проблемы с потенцией, слабая эрекция, снижение либидо³.
Эти симптомы могут возникать при заболеваниях не только предстательной железы, но и других органов мочеполовой системы. Если появляются хотя бы некоторые из этих признаков, нужно как можно быстрее обратиться к урологу.
При разных болезнях простаты характер болей и набор симптомов будут различаться. Существует три основных заболевания предстательной железы: простатит, доброкачественная гиперплазия и рак. Набор причин, вызывающих заболевания простаты, обширен (рис. 2).

Простатит
Простатит — воспаление предстательной железы. Оно может быть острым, возникающим из-за бактериальной инфекции, или хроническим (развивается как осложнение невылеченного острого простатита).
Острый простатит проявляется лихорадкой, ознобом, болью в пояснице, внизу живота или спины, в паховой области, частым мочеиспусканием и болями во время него. При остром простатите боли острые, резкие, их сложно терпеть. Спазмы могут усиливаться после опорожнения мочевого пузыря. Если простатит хронический, боли ноющие, тянущие, могут отдавать в задний проход, сохраняются подолгу.
Для лечения острого простатита уролог назначает антибиотики, а также лекарства, облегчающие симптомы болезни (жаропонижающие, обезболивающие и другие средства). Если сразу обратиться к врачу, острый простатит хорошо лечится, но если воспаление развивается или переходит в хроническую форму, эффективность терапии снижается (рис. 3). Хронический простатит плохо поддается лечению. Он не опасен для жизни, но снижает ее качество, периодически обостряется и со временем приводит к бесплодию и импотенции³.
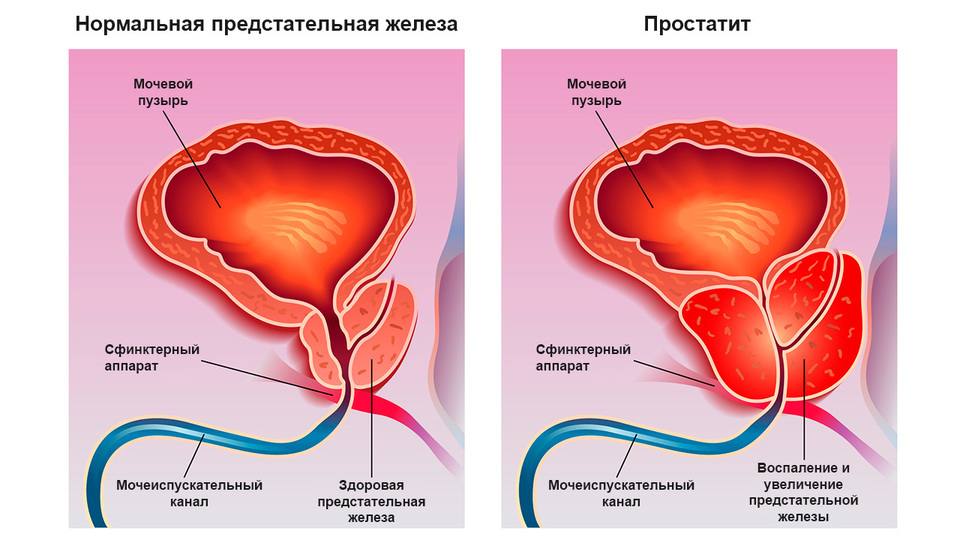
Доброкачественная гиперплазия предстательной железы
Доброкачественную гиперплазию предстательной железы также называют аденомой простаты. Это состояние, при котором ткани железы разрастаются, увеличиваются в объемах так, что железа сдавливает мочеиспускательный канал и это приводит к нарушению мочеиспускания (рис. 4). Это состояние развивается с возрастом. Его связывают с изменением гормонального фона по мере снижения сексуальной активности.
При аденоме простаты почти никогда нет болей, а основным признаком заболевания становятся проблемы с мочеиспусканием. Они нарастают постепенно.
- Сперва возникает небольшая задержка перед началом мочеиспускания, а струя становится слабой. Полное опорожнение мочевого пузыря требует небольшого напряжения мышц брюшного пресса.
- Далее позывы к мочеиспусканию становятся более частыми, но при этом полностью опорожнить мочевой пузырь трудно.
- Мочевой пузырь не опорожняется полностью, в нем постоянно остается некоторый объем мочи. Стенки мочевого пузыря начинают растягиваться. Процесс мочеиспускания становится длительным, часто прерывается, требует усилий.
- На конечной стадии в мочевом пузыре постоянно есть большой объем мочи, он сильно растянут, не может опорожняться. Моча начинает подкапывать, развивается недержание. На этой стадии внизу живота появляются боли, а также есть симптомы интоксикации, связанной с накоплением мочи. Работа почек нарушается.
Эти этапы аденома простаты проходит медленно. Заболевание может развиваться годами и даже десятилетиями. Оно постепенно снижает качество жизни, а также угрожает появлением рака простаты. Чтобы предупредить развитие осложнений и контролировать состояние предстательной железы, важно периодически проходить осмотры у уролога, а также обращаться к нему при появлении любых тревожных симптомов³.
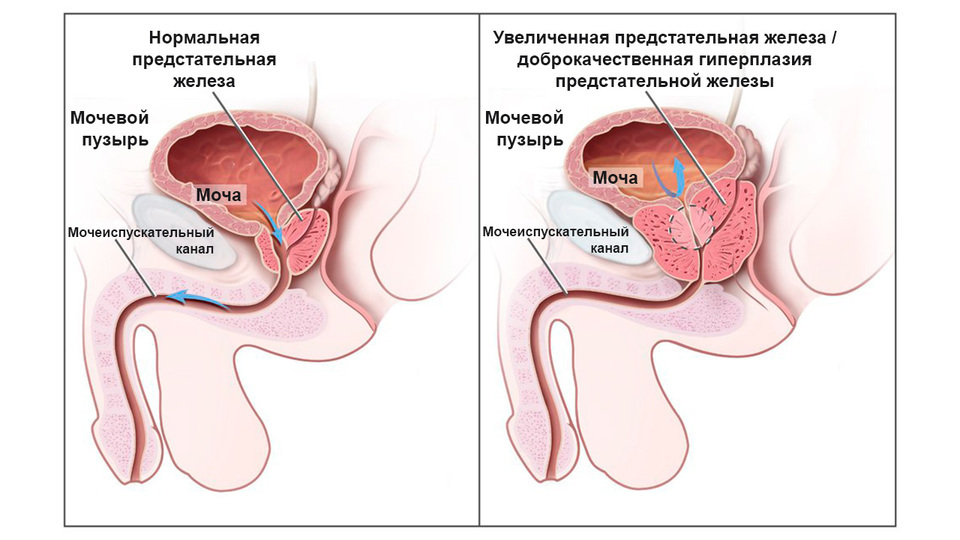
Рак предстательной железы
Рак предстательной железы — распространенное онкологическое заболевание. Чаще всего развивается в периферической зоне простаты. Факторами риска считаются пожилой возраст, неправильное питание, некоторые перенесенные вирусные инфекции, генетическая предрасположенность. Также рак может развиваться как осложнение аденомы простаты. Его симптомы чаще всего связаны с нарушениями мочеиспускания (частые позывы, неполное опорожнение мочевого пузыря, слабая струя). Также возможны боли в промежности (ощущаются как сильные спазмы). Симптомы рака предстательной железы появляются на поздних стадиях заболевания. На ранних стадиях рак прогрессирует бессимптомно (рис. 5.). Чтобы вовремя выявить его, необходимо периодически проходить осмотры у уролога и контролировать состояние простаты³.
Регулярно проходить скрининг рака предстательной железы рекомендуют мужчинам в возрасте от 55 до 69 лет. Это особенно важно, если мужчина входит в группу риска (при избыточном весе и/или в случаях, если у кровных родственников по мужской линии уже были случаи рака простаты). Для ранней диагностики можно сдавать анализ крови для определения опухолевого маркера ПСА (простатспецифический антиген). Уровень общего ПСА может повышаться не только в связи с развитием рака предстательной железы, но и при некоторых других состояниях, например, при инфекциях, простатите или аденоме. Поэтому если уровень общего ПСА повышен, нужно уточнить диагноз. Если есть подозрение на рак, можно сделать биопсию, однако эта процедура опасна тяжелыми осложнениями. Врач должен принимать решение о ее проведении вместе с пациентом, рассказав ему обо всех возможных рисках.
Для лечения рака простаты применяется несколько методов, включая лучевую, гормональную и химиотерапию, а также удаление опухоли. Обычно опухоль удаляется вместе с предстательной железой. После этого могут возникать осложнения: импотенция, эректильная и оргазмическая дисфункции, недержание мочи и другие.

Профилактика заболеваний простаты
Чтобы снизить риск болезней предстательной железы, не нужна специальная или сложная профилактика — достаточно вести здоровый образ жизни и периодически контролировать состояние мочеполовой системы.
Существует несколько рекомендаций по профилактике болезней простаты:
- Важно защищаться от инфекций. Для защиты от половых инфекций нужно использовать презерватив, занимаясь сексом. Также важно соблюдать правила мужской гигиены и прикасаться к половым органам только чистыми руками.
- Нужно исключить переохлаждение органов малого таза. Оно может быть причиной воспаления, а также нарушений мочеиспускания.
- Надо вести подвижный, активный образ жизни. Это особенно важно для мужчин с сидячей работой, для тех, кто мало ходит пешком и в основном ездит на машине. Ходьба, гимнастика и любая другая физическая активность препятствуют застою крови в органах малого таза и улучшают их работу.
Сохранить здоровье простаты поможет мужская интимная гимнастика:
- Расслабьте живот, глубоко вдохните и выдохните, одновременно сжимая, а затем расслабляя анальный сфинктер. Повторяйте в течение 2-4 минут.
- Чтобы стимулировать кровообращение, в течение одной минуты нужно массировать половой член пощипывающими движениями от головки до основания и обратно.
- Пробовать совершать несколько движений половым членом вверх-вниз и вправо-влево.
Эти упражнения можно повторять 2-3 раза в неделю. Они помогут укрепить мышцы тазового дна, улучшить кровообращение в малом тазу, снизить риск простатита и эректильной дисфункции.
- Секс должен быть регулярным. В числе факторов риска заболеваний простаты — редкий или нерегулярный секс, большие перерывы в сексуальной активности. Если они возникают, можно использовать мастурбацию. Каждая эякуляция заставляет простату работать, стимулирует кровообращение и обменные процессы.
Также нужно периодически проходить осмотры у уролога, даже если нет никаких поводов для беспокойства. Это особенно важно для мужчин старше 45 лет — для них такие осмотры должны быть регулярными (каждые три года или чаще).
Что такое массаж простаты и зачем он нужен?
Массаж простаты выполняется через задний проход и предполагает механическое воздействие на нее. Такой массаж может быть интимным, лечебным или диагностическим.
Интимный массаж применяется сексуальными партнерами и предполагает воздействие на заднюю поверхность железы (пальцами или предметами с доступом через анальное отверстие). Он может усиливать половое возбуждение, но при этом опасен травмами и занесением инфекции.
Диагностический и лечебный массаж проводятся в больнице врачом. Последний может использоваться при хроническом простатите. Он помогает восстановить проходимость протоков, улучшить отток секрета, стимулировать кровообращение, повысить мышечный тонус простаты.
В кабинете уролога
Для исследования простаты уролог проводит ректальный осмотр. Это неприятная процедура, но в норме она не причиняет боли. Мужчине нужно будет лечь на кушетку на бок или принять коленно-локтевую позу. Уролог наденет на руку одноразовую перчатку, смажет палец вазелином и введет его в задний проход, чтобы прощупать простату. Если нужно собрать секрет простаты для анализа, во время этой же процедуры врач массирует ее. Секрет выделяется через мочеиспускательный канал, и его достаточно собрать в стерильный контейнер. Также при осмотре, если есть подозрение на инфекцию, уролог возьмет мазок из уретры. Для этого в мочеиспускательный канал вводится специальный зонд.
Проходить профилактические осмотры у уролога очень важно, даже если нет никаких симптомов урологических заболеваний. Болезни предстательной железы, включая онкологию, могут развиваться незаметно и важно диагностировать их на раннем этапе. Они очень распространены — 80% мужчин старше 60 лет страдают от увеличения простаты, но подобные проблемы могут коснуться и молодого человека.
Заключение
Предстательная железа не является жизненно важным органом, но от ее здоровья зависит работа всей мочеполовой системы. Контролировать ее состояние особенно важно еще и потому, что рак простаты находится в числе самых распространенных среди мужчин онкологических заболеваний. Для такого контроля достаточно периодически проходить профилактические осмотры у уролога. Также важно сразу же обращаться к врачу, если появляются симптомы болезней простаты: трудности при мочеиспускании, боль внизу живота, нарушения эрекции.
Источники
- Prostate Gland. Prostate Cancer Foundation, 2018.
- Д. Ю. Пушкарь. Урология. М.: ГЭОТАР-Медиа, 2017.
- Mark Gurarie. The Anatomy of the Prostate. VeryWellHealth, 2020.
- Jennifer K. Nelson. Enlarged prostate: Does diet play a role? Mayo Clinic, 2020.
Предстательная железа (простата)
![]()
![]()
Читайте далее

Суперфуды в косметике: сочные коктейли для здоровья кожи и волос
Как суперфуды из питания попали в косметику, и что они могут сделать для вашей кожи и волос?
Опубликовано 13.09.2013 12:37, обновлено 27.06.2022 11:46
Читайте также
Аденома простаты: диагностика и лечение

Феномен данного заболевания — в отсутствие профилактики. Этот возрастной недуг в той или иной степени коснется более 85% мужчин после 70 лет. Другими словами, основной фактор, который становится причиной развития аденомы простаты — старение.
Аденома простаты без операции

Высокая вероятность хирургического вмешательства при аденоме простаты страшит многих мужчин. Однако не всегда этот диагноз – показатель для операции.
Воспаление аденомы простаты

Аденома простаты беспокоит каждого второго мужчину пожилого возраста. Как вовремя диагностировать болезнь и остановить ее развитие?
Аденома простаты: народное лечение

Народные средства в лечении аденомы простаты выполняют вспомогательную функцию и могут являться лишь дополнением к назначаемой врачом медикаментозной терапии
После ультразвукового исследования простаты пациент получает протокол, в котором указаны различные показатели, однако для неспециалиста эти данные ничего не говорят. Как же расшифровать полученный результат.
Где находится, как выглядит и на что похожа предстательная железа
Этот орган размером примерно с каштан или грецкий орех находится под мочевым пузырем. Простата состоит из двух симметричных частей, расположенных вокруг мочеиспускательного канала. Между ними находится перешеек, снабженный выступом – язычком, выходящим внутрь мочевого пузыря. Сзади орган граничит с прямой кишкой.
В простате может быть от 4 до 8 долек, состоящих из мелких желез, похожих на виноград. Эти образования выделяют жидкость – простатический секрет. Процесс контролируется гормоном тестостероном, вырабатываемым яичками.
Через простату проходят два семяпровода, доставляющих семенную жидкость из яичек. Во время семяизвержения предстательная железа зажимает проходящий через нее мочеиспускательный канал и не дает моче попасть в семя.
Все структуры железы хорошо видны при УЗ-диагностике, поэтому ультразвук широко применяется для выявления простатических патологий.

Чем отличается ТрУЗИ от ТаУЗИ
Оба варианта означают ультразвуковое обследование. Различается только метод его проведения:
- ТрУЗИ (трансректальное УЗИ) проводится через заднепроходное отверстие. Поскольку простата одной своей стороной выступает в прямую кишку и соприкасается с ней, осмотреть ее таким образом достаточно легко. Метод не применяется после «свежих» прямокишечных операций и при острых патологических патологиях – воспаленных геморроидальных узлах, болезненных трещинах заднего прохода, воспалении тканей, окружающих кишку, – парапроктите. В этом случае больного осматривают через кожу живота.
- ТаУЗИ (трансабдоминальное УЗИ) проводится через брюшную стенку. Низ живота смазывается гелем, и врач водит по коже датчиком, осматривая железу. Метод не применяется у пациентов с избыточным весом и большим количеством жира в этой области.
Простата при ТрУЗИ и ТаУЗИ видна с разных ракурсов, поэтому в протоколе указывается, как именно осматривался больной.
Характеристики применяемого оборудования
В бланке обязательно указывается тип применяемого оборудования, его модель, а также тип используемых датчиков. Такая информация нужна для профессионалов, которые поймут, насколько информативно полученное изображение.
Ультразвуковая аппаратура постоянно совершенствуется, поэтому в разных медучреждениях имеется техника, принадлежащая к различным поколениям. Вероятен вариант, что старый аппарат не обнаружит ряд патологий, поэтому ультразвуковое обследование желательно проводить на максимально современном оборудовании.
Для чего в протоколе указывается возраст пациента
Этот показатель нужен, чтобы врач мог рассчитать размеры простаты и понять природу изменений в органе. Железа состоит из основы – стромы – и железистых клеток, вырабатывающих простатическую жидкость. С возрастом строма становится более выраженной, а железистые клетки уменьшаются и становятся более редкими. Ухудшается кровообращение органа, внутри него могут появляться мелкие камни – кальцинаты.
У мужчин старше 45 лет намного чаще обнаруживаются изменения в железе, варьирующиеся от ее увеличения до рака. Поэтому простата возрастного и молодого пациента на УЗИ простаты значительно различается.
Физические характеристики железы, указываемые в протоколе
Форма, которая должна быть овальной и симметричной. Асимметрия и изменение конфигурации возникают при воспалительных процессах и опухолях. Поражение может быть односторонним, когда железа становится больше по размеру слева или справа, и двусторонним, при котором орган увеличивается равномерно.
Размеры. В среднем железа имеет габариты:
- Передне-задний – 1.5-2.5 см.
- Продольный и поперечный – 2.5-4.3 см.
По этим данным вычисляется объём. Для этого используется математическая формула расчета объема эллипса. Произведение длины, ширины и толщины органа умножают друг на друга, а затем на коэффициент 0.52. Вычисляется масса железы. Для этого полученный объем нужно умножить на 1.2.
В норме объем простаты у молодого человека составляет примерно 19-25 см куб. После 60 лет он может достигать 30 куб. и даже больше.
Получить более точные данные об объеме железы для определенного возраста можно по формуле Громова = 0,13 × возраст (лет) +16,4 = объем органа
Например, для 43 лет нормальный объем органа составит:
0,13 × 43 +16,4 = 21,99 куб. см
Небольшое отклонение от нормы вполне возможно, поскольку каждый мужчина имеет свои особенности строения организма.
Эти данные нужны, чтобы определить гиперплазию – разрастание предстательной железы, которое часто возникает после 45 лет, – и заподозрить опухоли, также сопровождающиеся увеличением органа.
Эхогенность. Под этим термином подразумевается способность тканей отражать ультразвуковые волны:
- Плотные образования хорошо отражают УЗ-волны, выглядят на экране светлыми и называются гиперэхогенными.
- Мягкие очаги и органы, участки содержащие жидкость, имеют темный цвет и считаются гипоэхогенными.
Предстательная железа, как и многие другие внутренние органы, выглядит на экране монитора тёмно-серой, то есть имеет среднюю эхогенность. Сверху простата покрыта плотной оболочкой, имеющей на УЗИ более светлый цвет. Внутри она рыхлее и, соответственно, темнее.
Запись в результатах УЗИ об увеличении эхогенности говорит о замещении железистой ткани жировой или соединительной. Это неблагоприятный процесс, при котором орган хуже выполняет свои функции. Такая патология часто развивается на фоне воспаления и является последствием недолеченных гонореи, трихомониаза, хламидиоза и других половых инфекций. Соединительнотканное перерождение простаты ведет к бесплодию.
Пониженная эхогенность указывает на воспалительный процесс – простатит. Обнаруженные на фоне воспаленной железы тёмные гиперэхогенные структуры свидетельствуют о развившемся гнойном процессе и образовании гнойников (абсцессов простаты).
Эхогенность участков органа при опухолях может повышаться или понижаться в зависимости от свойств и структуры возникшего новообразования. Иногда обнаруживается несколько опухолевых очагов, создающих пеструю картину.
Патологические процессы, обнаруживаемые в железе
Доброкачественная гиперплазия. При этом заболевании размеры простаты увеличиваются, а сама она, разрастаясь, может перекрывать мочеиспускательный канал и мешать отхождению урины. Такое состояние может быть:
- Диффузным – железа равномерно увеличивается в размерах, приобретая шарообразную форму. На УЗИ её структура не имеет явно выраженных светлых или тёмных очагов.
- Узловым – при этой форме болезни обнаруживаются узлы, имеющие повышенную плотность. На УЗИ они выглядят как более светлые участки разного размера.
Камни предстательной железы, образующиеся при калькулезном простатите, на УЗИ видны как небольшие светлые образования.
Участки воспаления имеют более темный цвет. Иногда в них обнаруживаются гнойники (абсцессы) разного размера. В процесс могут вовлекаться находящиеся рядом семенные пузырьки, которые тоже становятся увеличенными и неоднородными по структуре.
Кисты – образования, заполненные жидкостью. Выглядят как темные пятна на фоне более светлой железистой ткани.
При раке железа увеличивается, а ее контуры теряют четкость. Чаще всего злокачественные опухоли обнаруживаются в краевой части железы. В середине органа они возникают только в 5% случаев. Иногда рак сливается с доброкачественной гиперплазией и его сложно обнаружить. Таким больным проводятся дополнительные обследования, уточняющие природу образования.
УЗИ простаты – удобный, информативный и недорогой метод диагностики самых распространенных болезней органа. Этот вид диагностики рекомендуется проходить раз в год всем мужчинам, особенно старше 45 лет.
Обязательно нужно пройти такую диагностику после лечения половых инфекций. На фоне ЗППП часто развивается простатит и даже могут образовываться гнойники внутри тканей.

Что делать, если результат УЗИ простаты оказался неблагоприятным
В этом случае нужно обратиться к врачу-андрологу, который назначит дополнительную диагностику, поставит диагноз и проведет лечение выявленных болезней. Пациенту назначаются:
- Биопсия простаты – процедура, во время которой из органа берутся небольшие фрагменты тканей для клеточного анализа. После ее проведения можно узнать тип опухоли и ее злокачественность.
- УЗИ малого таза и брюшной полости, проводимое при подозрении на раковые опухоли. Метод выявляет возможные метастазы.
- УЗИ мочевого пузыря назначается при застойных явлениях, вызванных пережатием уретры увеличенной простатой и нарушением оттока урины. Определяется остаточная моча – количество урины, оставшееся после мочеиспускания. В норме ее должно быть не более 50 мл.
- Кровь на ПСА – простатический антиген. Увеличение показателя более 4,0 нг/мл – плохой признак, указывающий на возможное развитие рака.
- Анализы на определение ЗППП. Наиболее информативно исследование Андрофлор, выявляющее все инфекции, в том числе скрытые и вялотекущие.
При обнаружении воспалительных и инфекционных процессов больным назначают противовоспалительные средства и антибиотики. При разрастании железы показаны препараты, уменьшающие объем увеличенной простаты и улучшающие мочеиспускание. Во время лечения проводятся повторные УЗИ и сдача анализов для выявления эффективности лечебных мероприятий.
![]()
Как устроена предстательная железа?
Предстательная железа — это непарный орган репродуктивной системы у мужчин. Основная функция простаты — вырабатывать простатический секрет. Он выбрасывается в мочеиспускательный канал во время эякуляции и нужен для активации сперматозоидов.
В различные периоды жизни мужчины структура предстательной железы изменяется. До начала полового созревания предстательная железа состоит в основном из мышечных волокон и имеет малый размер. На пике половой активности начинает преобладать железистый компонент. К пожилому возрасту объем железы уменьшается.
Таким образом, предстательная железа имеет смешанное строение. Чтобы не допустить смешивания мочи и спермы, во время эякуляции мышечные волокна простаты сокращаются. А железы простаты выделяют специальное вещество, которое разжижает сперму и поддерживает способность сперматозоидов к движению.
Как выглядит предстательная железа и какие у нее размеры?
Нормальная предстательная железа половозрелого мужчины имеет массу приблизительно 20 граммов, она около 3-х см в длину, 4-х см в ширину и 2-х см в глубину. По форме и размеру она напоминает каштан.
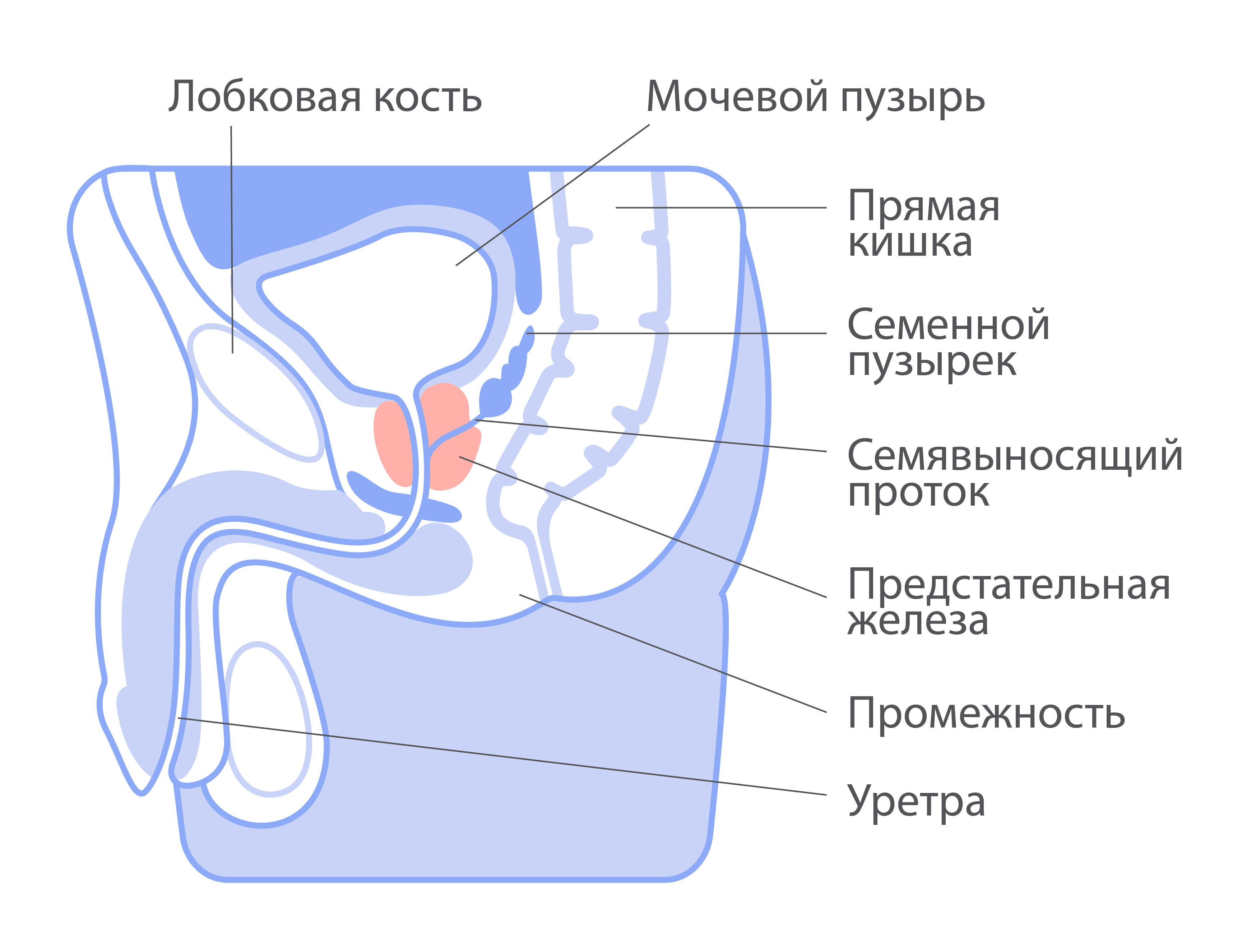
Из каких частей состоит предстательная железа?
Простату разделяют на три зоны: центральная зона, периферическая зона и переходная зона. Также выделяют правую и левую доли, которые соединены между собой средней долей (перешейком).
Тело предстательной железы состоит из гладких мышц. Они составляют от четверти до половины ее объема. В мышечные волокна вплетаются эластичные соединительнотканные волокна. В ткани железы располагаются 30–50 извитых канальцев, в которых вырабатывается секрет.
Через предстательную железу проходят мочеиспускательный канал (уретра) и два семявыносящих протока. Уретра служит для выведения мочи при мочеиспускании. Также через нее выводится эякулят в процессе семяизвержения.
Семявыносящие протоки нужны для того, чтобы доставлять сперматозоиды из яичек в уретру. Сперматозоиды, образовавшиеся в семенных канальцах яичка, незрелые и неподвижные. Именно в уретре они смешиваются с с секретом предстательной железы и «активируются». Читайте подробнее о функциях предстательной железы в этой статье.
Что окружает предстательную железу?
Предстательная железа находится в малом тазу. Она располагается чуть ниже мочевого пузыря и окружает начальную часть уретры. Сзади она ограничена прямой кишкой, спереди — костями таза (лобковым сочленением), снизу расположены мышцы промежности (их еще называют мочеполовой диафрагмой). Предстательная железа покрыта капсулой из соединительной ткани.
Онколог-маммолог, выпускник Высшей школы онкологии
12 сентября 2022
Пройдите короткий тест, получите рекомендации и график обследований.
пройти тест
Помочь фонду «Не напрасно» прямо сейчас
Все собранные средства идут на оплату экспертов, задействованных в консультациях, и на работу сервиса. Поддерживая системные проекты — образование талантливых врачей, просвещение широкой аудитории, внедрение технологий скрининга рака, — вы можете внести вклад в спасение сотен и тысяч людей в России и обеспечить помощь себе и своим близким, если в ней возникнет необходимость.
Строение и функции
Предстательная железа (простата) – это непарная экзокринная железа половой системы мужчины, анатомическое расположение которой определяет ее основные функции. Она имеет определенную форму, с возрастом увеличивается и частично меняет свой вид. ПЖ представлена железистой и мышечной тканью. Железистая ткань является источником формирования гормонов и простатического сока, мышечная ткань отвечает за регулировку просвета уретры.

Объем органа во многом зависит от телосложения мужчины. В среднем размеры ПЖ следующие: ширина – 3,5 см, длина – 3 см, толщина – около 2 см. Ее масса не превышает 20 г. Простата напоминает по своей форме грецкий орех или крупный каштан. Его более узкий полюс расположен вокруг начальной части мочеиспускательного канала, а более широкий примыкает к нижней части мочевого пузыря и охватывает его шейку.
Функции простаты многогранны:
-
отвечает за стабильные сексуальные возможности
-
препятствует забросу семенной жидкости в мочевой пузырь
-
выделяет жидкость, которая разжижает сперму и создает благоприятные условия для активности сперматозоидов
-
помогает контролировать процесс мочеиспускания
-
защищает половой тракт мужчины от инфекций. Она не допускает проникновение попадающих из мочевыводящего канала микроорганизмов в верхние мочевые пути, защищая их от различных заболеваний инфекционного характера.
Любые патологии органа приводят к нарушению процесса мочеиспускания, развитию воспаления, проблемам в половой сфере. Особенность строения предстательной железы в том, что через нее проходит мочеточник. Патологии простаты приводят к нарушению процесса освобождения мочевого пузыря.
Заболевания предстательной железы:
Простатит – болезнь, связанная с воспалением предстательной железы. Может развиться у мужчин любого возраста, носить хронический или острый характер течения. Воспаленные ткани простаты меняют свою структуру, нарушаются функции клеток и ПЖ в целом, из-за чего могут возникнуть серьезные последствия, вплоть до снижения либидо и импотенции, возникновения синдрома хронической тазовой боли, расстройства мочеиспускания. Именно поэтому важно вовремя заметить симптомы и обратиться за помощью к врачу. Все дело в том, что мужчины очень боятся данного заболевания, и даже заметив симптомы, пытаются оттянуть момент похода к врачу.
В зависимости от причины происхождения, различают нескольких видов простатита: бактериальный простатит – начинается на фоне проникновения в ткани предстательной железы инфекции, диагностика такого вида простатита чаще происходит у молодых и пожилых мужчин. Застойный простатит – вызван малоподвижным образом жизни, отсутствием у мужчин регулярной половой жизни и травмами малого таза, часто сопровождается проникновением инфекции, и тогда простатит становится смешанного вида. Калькулезный простатит – развивается как следствие невылеченной хронической формы течения заболевания, чаще такой простатит встречается у мужчин пожилого возраста. По форме протекания простатит делится на острый и хронический. Диагностика острой формы заболевания происходит редко, лечение должно проводиться только в стационарных условиях, потому что простатит протекает с выраженными симптомами. Простатит хронической формы отличается «вялой» клинической картиной, периодическими ремиссиями, полным отсутствием специфических симптомов и быстрой трансформацией в серьезные проблемы – перерождение здоровых клеток предстательной железы в злокачественные, прекращение выработки секрета, снижение содержания в секрете сперматозоидов.
Основной причиной появления простатита является попадание в железу инфекций, чему способствует анатомическое строение предстательной железы. Инфекция может попасть в простату из мочеиспускательного канала, прямой кишки, лимфатическим и гематогенным путем.
Если простатит диагностируется своевременно, то лечение длится всего 2 недели, после чего мужчине нужно будет лишь соблюдать рекомендации врача и периодически проходить контрольное обследование. В таком случае никаких осложнений после перенесенного воспаления простаты не будет – репродуктивные способности сохраняются в полном объеме, даже если простатит протекал с острой симптоматикой.
Аденома простаты – доброкачественная опухоль, образованная в результате разрастания железистой или соединительной тканей. На первых этапах развития у мужчины аденомы простаты в тканях органа появляются узелки, которые начинают постепенно расти. Время роста длительное. Иногда в течение ряда лет мужчина не догадывается о проблеме, не обращает внимания на первые симптомы. Увеличенная железа сдавливает мочевыделительный канал, мешает освобождению мочевого пузыря. Ткань разрастается в направлении к кишечнику или ко дну мочевого пузыря, постепенно в него вклиниваясь.
Аденому простаты не стоит путать с простатитом – это два разных заболевания. Первое характеризуется ростом ткани, второе – развитием воспалительного или инфекционного процесса.
Рак предстательной железы (активная ссылка на пост о раке предстательной железы) (РПЖ) – наиболее часто встречающаяся злокачественная опухоль мочеполовой системы у мужчин. Это медленнорастущая опухоль, которая на начальной стадии часто не проявляется никакими симптомами.
Выделяют 4 стадии рака простаты:
- 1 и 2 стадия – локализованный рак простаты, когда опухоль ограничена капсулой простаты и не распространяется за ее пределы.
- 3 стадия – местно-распространенный рак простаты, когда опухоль прорастает в жировую клетчатку вокруг простаты или в семенные пузырьки.
- 4 стадия – метастатический рак простаты, имеются опухолевые отсевы в регионарные лимфатические узлы и/или в другие органы.
Причины заболеваний
-
особенности строения предстательной железы, которое способствует застою секрета в выводных протоках желез
-
особенности строения венозной сети предстательной железы, которое приводит к застою крови
-
нарушения гормонального фона (врожденная патология, неконтролируемый прием гормональных препаратов)
-
особенности строения нервно-рефлекторных связей с прямой кишкой и мочевым пузырем
-
возрастные изменения самой простаты и уровня содержания гормонов
-
врожденное снижение иммунитета
-
хронические травмы промежности (длительная верховая езда, езда на велосипеде)
-
чрезмерно активная половая активность
-
хронические нарушения стула – в частности, запоры, при которых у мужчин возникает потребность сильно тужиться
-
курение и алкоголь
-
инфекции, передающиеся половым путем (хламидиоз, уреаплазмоз, кандидоз, микоплазмоз, гонорея, трихомониаз и др.)
-
тяжелые формы ангины, пневмонии, гриппа, когда простатит напрямую связан с проникновением в ткани железы инфекционных агентов
-
вирусы (чаще всего урогенитальный герпес – вирус герпеса 2-го типа, реже вирус гриппа)
-
иммунологические нарушения (в том числе аутоиммунные)
-
химическое поражение вследствие рефлюкса мочи
-
нейрогенные нарушения
-
переохлаждение области малого таза
-
сидячий или малоподвижный образ жизни
-
нервное и физическое перенапряжение
-
нерегулярная половая жизнь
-
избыточная масса тела
-
наследственность, наличие болезни у близких родственников
Симптомы заболеваний
Симптомы напрямую зависят от того, какой вид простатита начинает развиваться в тканях предстательной железы: бактериальный простатит – высокая температура тела, присутствие в моче крови или гноя, проблемы с мочеиспусканием (тонкая и слабая струя, «капельный» выход мочи), острая боль в области промежности, плохое общее самочувствие. Калькулезный простатит – слабая эрекция или ее полное отсутствие, кровь в моче, такие симптомы простатита чаще присутствуют у мужчин 50 лет и старше. Застойный простатит – дискомфортные ощущения в области промежности и яичках, частичное или полное отсутствие эрекции, неправильное мочеиспускание. Простатит хронической формы течения отличается «смазанной» клинической картиной, все симптомы невыраженные и могут беспокоить периодически. Но если у мужчин в течение 2-3 месяцев появляются боли в паху и яичках, повышается общая температура тела, снижается половое влечение, то это значит, что нужно обратиться к врачу, подтвердить диагноз «хронический простатит» и пройти лечение. Стоит знать следующие нюансы: симптомы простатита у мужчин в 50 лет – это ослабление эрекции и ощущение тяжести в паху, а вот болевой синдром может полностью отсутствовать. Симптомы простатита у мужчин в 30 лет всегда проявляются остро, и первым признаком является нарушение мочеиспускания: увеличенная простата сдавливает мочевой пузырь, и у мужчин просто не получается сходить в туалет. Симптомы простатита у мужчин в 60 лет могут отсутствовать – в таком возрасте простатит часто носит хронический характер, но может беспокоить полное отсутствие эрекции. Эффективное лечение врач сможет назначить только после диагностики заболевания – простатит часто имеет симптомы других заболеваний мочеполовой системы, таких как рак предстательной железы.
Диагностика:
Учитывая, что разные заболевания имеют преимущественно одинаковые симптомы, поставить точный диагноз на основании только жалоб пациента практически невозможно. Поэтому назначаются дополнительные обследования:
Осмотр врача-уролога:
- пальцевое ректальное обследование.
Анализы:
- лабораторное исследование секрета предстательной железы
- анализ на выявление/отсутствие инфекций, передающихся половым путем
- Простатспецифический антиген (ПСА) – органоспецифический показатель, однако не считается специфическим для рака, поскольку его уровень может быть повышенным при доброкачественной гиперплазии предстательной железы (ДГПЖ), простатите. Уровень ПСА ниже, чем 4 нг/мл не исключает наличие клинически значимого РПЖ.
Ультразвуковые исследования:
- УЗИ простаты
- УЗИ органов малого таза
- УЗИ мошонки и пениса
Биопсия предстательной железы
Это процедура взятия небольших кусочков ткани предстательной железы. Во время биопсии доктор будет использовать метод УЗИ, чтобы взять ткани из нужных областей предстательной железы. После биопсии полученные кусочки ткани отдаются на гистологическое исследование, где их изучают под микроскопом на наличие аномальных клеток
Показанием для биопсии ПЖ служит уровень ПСА > 4 нг/мл и/или изменения, выявленные при пальцевом ректальном исследовании или УЗИ.
Компьютерная и магнитно-резонансная томография:
При подтвержденном РПЗ для планирования хирургического вмешательства или дальнейшей тактики лечения необходимо дополнительно провести радиологические исследования, такие как КТ и МРТ.
- МРТ органов малого таза. Наиболее эффективный метод локального стадирования заболевания
- КТ рекомендована для исключения метастазов в лёгкие, лимфоузлы средостения и выявления изменений в других солидных органах. КТ помогает установить стадию заболевания.
Остеосцинтиграфия с 99mTc является наиболее часто применяемым методом диагностики метастазов РПЖ в кости.
Может понадобится привлечение узких специалистов для исключения или подтверждения сопутствующих заболеваний.
Рак предстательной железы диагностируется преимущественно на I-II стадиях– 42,6%, на III стадии– 22,4%, на IV стадии– 22,3%. Прогноз заболевания определяется его стадией – 5 лет с момента диагностики проживут около 100% с I-II стадией, около 100% с III стадией, 31% с IV стадией.
Пренебрежение правильной диагностикой может привести к тому, что простатит перерастет в запущенную форму, и традиционное лечение не поможет. Опасность заключается в высокой вероятности развития рака простаты и полного бесплодия.
Лечение
Симптомы простатита у мужчины и его лечение напрямую связаны, потому что при назначении терапии врач в первую очередь должен облегчить общее состояние пациента. Лучшее лечение – комплексное, и поэтому чтобы простатит как можно быстрее купировать, нужно точно соблюдать рекомендации лечащего врача. У мужчин часто присутствует сильная боль, а значит лечение нужно начинать с обезболивающих препаратов. Как только признаки заболевания станут менее выраженными, предстоит восстанавливать половую активность. Простатит гораздо быстрее вылечится, если обеспечить регулярный дренаж предстательной железы и не допускать даже небольшого застоя секрета в ее тканях.
Лечится ли отсутствие эрекции на фоне простатита? Да, при таких жалобах врач назначает специфические лекарственные средства, которые улучшают кровоснабжение полового органа и очищают сосуды предстательной железы от шлаков и токсинов. Если симптомы простатита выявлены у мужчин 40 лет, то дополнительных препаратов для восстановления эрекции не понадобится – как только воспалительный процесс купируется, все половые способности восстановятся. А вот если причиной простатита у мужчин 30 лет стали венерические заболевания (инфекции, передающиеся половым путем), то для восстановления сексуальной активности нужно будет пройти дополнительное лечение и выявленной инфекции.
Если лечение медикаментами не дает положительных результатов, простатит протекает в хронической форме с частыми рецидивами, это повод провести хирургическое вмешательство. Операция может быть двух видов: трансуретральная резекция – хирург удаляет ткани предстательной железы, которые поразил простатит; простатэктомия – простатит представляет реальную опасность для жизни мужчины, поэтому ему полностью удаляют и простату, и семенные пузырьки с прилегающими тканями. Операции не проводятся в молодом возрасте, потому что это может привести к полному бесплодию – простатит лечится терапевтическими методами, в дополнение к медикаментам могут быть назначены физиотерапевтические процедуры. Сколько продлится лечение простатита, зависит от стадии и формы заболевания, степени запущенности. Обычно это 2 недели, но показатель очень усредненный. Полностью вылечить простатит можно, важно только вовремя обратиться к врачу.
Лечение рака простаты является мультимодальным и включает в себя следующие опции: хирургическое удаление (открытая и лапароскопическая радикальная простатэктомия), лучевую терапию, гормональную терапию, химиотерапию, таргетную и иммунотерапию. Тактика лечения зависит от стадии заболевания по системе TNM и прогноза жизни пациента.
Описывая лечение рака простаты пациенту, важнее всего ответить на следующие вопросы:
- возможно ли полное излечение на данной стадии рака простаты?
- какой способ максимально безопасен для конкретного пациента?
- какое лечение обеспечит максимально продолжительную жизнь пациента с сохранением хорошего качества жизни?
Первое место в радикальном лечении злокачественного заболевания простаты занимает хирургическое вмешательство. Если опухоль не вышла за пределы простаты, если нет отдаленных метастазов, то вероятность избавления пациента от опухоли путем хирургического удаления предстательной железы очень высока.
Записаться на прием к врачу-урологу ЕРЦ
В «Европейском Радиологическом Центре» Вы можете получить комплексную диагностику, сдать все необходимые анализы и получить квалифицированное лечение данного заболевания. Прием ведет врач онкоуролог-хирург высшей категории с большим опытом работы с заболеваниями простаты Налбандян Тарон Альбертович.
Записаться на прием можно по телефону: +38 (099) 915-10-40