Как правильно пишется слово «сколиоз»
сколио́з
сколио́з, -а
Источник: Орфографический
академический ресурс «Академос» Института русского языка им. В.В. Виноградова РАН (словарная база
2020)
Делаем Карту слов лучше вместе

Привет! Меня зовут Лампобот, я компьютерная программа, которая помогает делать
Карту слов. Я отлично
умею считать, но пока плохо понимаю, как устроен ваш мир. Помоги мне разобраться!
Спасибо! Я стал чуточку лучше понимать мир эмоций.
Вопрос: панголин — это что-то нейтральное, положительное или отрицательное?
Ассоциации к слову «сколиоз»
Синонимы к слову «сколиоз»
Предложения со словом «сколиоз»
- При сколиозе позвоночника также с одной стороны мышцы сжаты, а с другой – слабы и растянуты.
- – На что следует обратить основное внимание при воспитании ребёнка, чтобы избежать развития сколиоза?
- У взрослых людей причиной сколиоза могут быть остеохондроз, травмы или тяжёлые инфекции, поражающие костную систему, такие как туберкулёз, сифилис и др.
- (все предложения)
Значение слова «сколиоз»
-
Сколио́з (греч. σκολιός — «кривой», лат. scoliōsis) — трёхплоскостная деформация позвоночника у человека. Искривление может быть врождённым, приобретённым и посттравматическим. (Википедия)
Все значения слова СКОЛИОЗ
Отправить комментарий
Дополнительно
![]()
Слова русского языка,
поиск и разбор слов онлайн
сколиоз
Правильно слово пишется: сколио́з
Ударение падает на 3-й слог с буквой о.
Всего в слове 7 букв, 3 гласных, 4 согласных, 3 слога.
Гласные: о, и, о;
Согласные: с, к, л, з.
Номера букв в слове
Номера букв в слове «сколиоз» в прямом и обратном порядке:
- 7
с
1 - 6
к
2 - 5
о
3 - 4
л
4 - 3
и
5 - 2
о
6 - 1
з
7
Русский[править]
Морфологические и синтаксические свойства[править]
| падеж | ед. ч. | мн. ч. |
|---|---|---|
| Им. | сколио́з | сколио́зы |
| Р. | сколио́за | сколио́зов |
| Д. | сколио́зу | сколио́зам |
| В. | сколио́з | сколио́зы |
| Тв. | сколио́зом | сколио́зами |
| Пр. | сколио́зе | сколио́зах |
ско—ли—о́з
Существительное, неодушевлённое, мужской род, 2-е склонение (тип склонения 1a по классификации А. А. Зализняка).
Корень: —.
Произношение[править]
- МФА: [skəlʲɪˈos]
Семантические свойства[править]

Значение[править]
- мед. дугообразное искривление позвоночника во фронтальной плоскости ◆ Отсутствует пример употребления (см. рекомендации).
- мед. то же, что сколиотическая болезнь — прогрессирующее диспластическое заболевание растущего позвоночника детей ◆ Отсутствует пример употребления (см. рекомендации).
- разг. сутулость, функциональный кифоз ◆ Отсутствует пример употребления (см. рекомендации).
Синонимы[править]
- искривление позвоночника
- идиопатический сколиоз, сколиотическая болезнь
- сутулость
Антонимы[править]
- —
- —
- ?
Гиперонимы[править]
- заболевание, дефект, искривление
- заболевание
- осанка, кифоз
Гипонимы[править]
- ?
- —
- ?
Родственные слова[править]
| Ближайшее родство | |
|
Этимология[править]
Происходит от лат. scoliosis, из др.-греч. σκολιός «кривой».
Фразеологизмы и устойчивые сочетания[править]
Перевод[править]
| искривление позвоночника | |
|
| сколиотическая болезнь | |
| стутулость | |
Библиография[править]
Сколиоз

Сколиоз – это стойкое искривление позвоночника вбок относительно своей оси (во фронтальной плоскости). В процесс вовлекаются все отделы позвоночника, потому к боковому искривлению в последующем присоединяется искривление в переднезаднем направлении и скручивание позвоночника. По мере прогрессирования сколиоза возникает вторичная деформация грудной клетки и таза, сопровождающаяся нарушением функции сердца, легких и тазовых органов. Патология диагностируется по данным осмотра и рентгенографии. Лечение может быть как консервативным, так и оперативным.
Общие сведения
Сколиоз – это сложная стойкая деформация позвоночника, сопровождающаяся, в первую очередь, искривлением в боковой плоскости с последующим скручиванием позвонков и усилением физиологических изгибов позвоночника. При прогрессировании сколиоза развивается деформация грудной клетки и костей таза с сопутствующим нарушением функции органов грудной полости и тазовых органов.
Самыми опасными периодами в отношении развития и прогрессирования сколиоза являются этапы интенсивного роста: от 4 до 6 лет лет и от 10 до 14 лет. При этом следует быть особенно внимательными к здоровью ребенка на этапе полового созревания, которое у мальчиков происходит в 11-14 лет, а у девочек в 10-13 лет. Риск усугубления сколиотической деформации увеличивается в тех случаях, когда к началу этих периодов у ребенка уже есть рентгенологически подтвержденная первая степень сколиоза (до 10 градусов).
Сколиоз не следует путать с обычным нарушением осанки. Нарушение осанки можно исправить с помощью обычных физических упражнений, обучения правильной посадке за столом и других подобных мероприятий. Сколиоз же требует специального комплексного систематического лечения в течение всего периода роста пациента.

Сколиоз
Причины сколиоза
Патология относится к группе деформаций, возникающих в период роста (то есть, в детстве и юности). На первом месте по распространенности с большим отрывом находится идиопатический сколиоз – то есть, сколиоз с неустановленной причиной. Он составляет около 80% от общего числа случаев. При этом девочки болеют сколиозом в 4-7 раз чаще мальчиков. В оставшихся 20% случаев наиболее часто выявляется сколиоз вследствие врожденных деформаций позвоночника, обменных нарушений, заболеваний соединительной ткани, тяжелых травм и ампутаций конечностей, а также значительной разницы в длине ног.
Классификация
В вертебрологии, травматологии и ортопедии существует несколько классификаций сколиоза. Можно выделить две большие группы: структурный сколиоз и неструктурный сколиоз. В отличие от структурного, при неструктурном наблюдается обычное боковое искривление позвоночника, не сопровождающееся стойкой патологической ротацией позвонков.
С учетом причин развития неструктурные сколиозы делятся на:
- Осаночные сколиозы – возникшие вследствие нарушения осанки, исчезающие при наклонах кпереди и проведении рентгенографии в лежачем положении.
- Рефлекторные сколиозы – обусловленные вынужденной позой пациента при болевом синдроме.
- Компенсаторные сколиозы – возникшие вследствие укорочения нижней конечности.
- Истерические сколиозы – имеют психологическую природу, встречаются крайне редко.
Структурные сколиозы также подразделяются на несколько групп с учетом этиологического фактора:
- Травматические – обусловленные травмами опорно-двигательного аппарата.
- Рубцовые – возникшие вследствие грубых рубцовых деформаций мягких тканей.
- Миопатические – обусловленные болезнями мышечной системы, например, миопатией или прогрессирующей мышечной дистрофией.
- Нейрогенные – возникающие при нейрофиброматозе, сирингомиелии, полиомиелите и т. д.
- Метаболические – обусловленные нарушениями обмена и нехваткой определенных веществ в организме, могут развиваться, например, при рахите.
- Остеопатические – возникшие вследствие врожденной аномалии развития позвоночника.
- Идиопатические – причину развития выявить невозможно. Такой диагноз выставляется после исключения остальных причин возникновения сколиоза.
С учетом времени возникновения идиопатические сколиозы делятся на:
- Инфантильные – развившиеся в 1-2 годы жизни.
- Ювенильные – возникшие между 4-6 годами жизни.
- Подростковые (адолесцентные) – появившиеся между 10 и 14 годами жизни.
По форме искривления все сколиозы делятся на три группы: C-образные (один боковой изгиб), S-образные (два боковых изгиба) и Z-образные (три боковых изгиба). Последний вариант встречается крайне редко.
С учетом места расположения искривления позвоночника выделяют:
- Шейно-грудные (с вершиной искривления на уровне III-IV грудных позвонков).
- Грудные (с вершиной искривления на уровне VIII-IX грудных позвонков).
- Грудо-поясничные (с вершиной искривления на уровне XI-XII грудных позвонков).
- Поясничные (с вершиной искривления на уровне I-II поясничных позвонков).
- Пояснично-крестцовые (с вершиной искривления на уровне V поясничного и I-II крестцовых позвонков).
И, наконец, с учетом течения различают прогрессирующий и непрогрессирующий сколиозы.

КТ ОГК. Выраженная левосторонняя сколиотическая деформация грудо-поясничного перехода.
Симптомы сколиоза
На начальных стадиях патология протекает бессимптомно, поэтому следует обращать внимание на следующие признаки: одно плечо находится выше другого; когда ребенок стоит, прижав руки к бокам, расстояние между рукой и талией различается с двух сторон; лопатки расположены несимметрично – на вогнутой стороне лопатка находится ближе к позвоночнику, ее угол выпирает; при наклоне кпереди становится заметным искривление позвоночника.
Классификация сколиозов, разработанная Чаклиным и использующаяся на территории России, была составлена с учетом как клинических, так и рентгенологических признаков, поэтому на нее можно ориентироваться при выявлении симптомов заболевания. Она включает в себя 4 степени:
- 1 степень – угол до 10 градусов. Определяются следующие клинические и рентгенологические признаки: сутуловатость, опущенная голова, асимметричная талия, разная высота надплечий. На рентгеновских снимках – легкая тенденция к торсии позвонков.
- 2 степень – угол от 11 до 25 градусов. Выявляется кривизна позвоночника, не исчезающая при смене положения тела. Половина таза на стороне искривления опущена, треугольник талии и контуры шеи асимиетричны, в грудном отделе на стороне искривления имеется выпячивание, в поясничном – мышечный валик. На рентгенограмме – торсия позвонков.
- 3 степень – угол от 26 до 50 градусов. В дополнение ко всем признакам сколиоза, характерным для 2 степени, становятся заметными выпирающие передние реберные дуги и четко очерченный реберный горб. Мышцы живота ослаблены. Наблюдаются мышечные контрактуры и западание ребер. На рентгеновских снимках – резко выраженная торсия позвонков.
- 4 степень – угол более 50 градусов. Резкая деформация позвоночника, все выше перечисленные признаки усилены. Значительное растяжение мышц в области искривления, реберный горб, западание ребер в зоне вогнутости.
Диагностика
Физикальное обследование
При выявлении симптомов сколиоза следует обратиться к детскому ортопеду, чтобы он провел детальное обследование и при подтверждении диагноза назначил соответствующее лечение. Обследование пациента, страдающего сколиозом, в условиях мед. учреждения включает в себя подробный осмотр в положении стоя, сидя и лежа для выявления перечисленных выше признаков.
В положении стоя проводится измерение длины нижних конечностей, определяется подвижность голеностопного, коленного и тазобедренного суставов, измеряется кифоз, оценивается подвижность поясничного отдела позвоночника и симметричность треугольников талии, определяется положение надплечий и лопаток. Также производится осмотр грудной клетки, области живота, таза и поясницы. Оценивается мышечный тонус, выявляются мышечные валики, деформация ребер и т. д. В положении сгибания определяется наличие или отсутствие асимметрии позвоночника.
В положении сидя проводится измерение длины позвоночника и определение степени поясничного лордоза, выявляются боковые искривления позвоночника и отклонения туловища. Производится оценка положения таза вне зависимости от положения нижних конечностей. В положении лежа оценивается изменение искривления дуги позвоночника, исследуются мышцы живота и внутренние органы.
Рентгенография
Основным инструментальным методом диагностики сколиоза позвоночника является рентгенография позвоночника. При подозрении на сколиотическое искривление рентгеновское исследование необходимо проводить не реже 1-2 раз в год. Первичная рентгенограмма может проводиться в положении стоя. В последующем рентгеновские снимки выполняются в двух проекциях в положении лежа с умеренным растягиванием – это дает возможность оценить истинную деформацию.
При изучении рентгенограмм больных сколиозом проводится измерение углов искривления с использованием специальной методики, предложенной Коббом. Для того чтобы рассчитать угол искривления, на прямую рентгенограмму наносят две линии, проходящие параллельно замыкательным пластинкам нейтральных (не участвующих в искривлении) позвонков, а затем измеряют угол, образованный этими линиями.
Кроме того, на рентгеновском снимке при сколиозе выявляют следующие особенности:
- Базальные неискривленные позвонки, которые являются основанием для искривленной части позвоночника.
- Кульминационные позвонки, расположенные на самой высокой точке дуги искривления (как основного, так и вторичного, если оно есть).
- Скошенные позвонки, которые находятся в местах перехода между основным искривлением и противоискривлением.
- Промежуточные позвонки, расположенные между скошенными и кульминационными позвонками.
- Нейтральные позвонки – недеформированные позвонки, не участвующие в процессе бокового искривления.
При необходимости выполняют снимки в специальных укладках для измерения торсии (скручивание вдоль оси тела позвонка) и ротации (разворота позвонков друг относительно друга). Торсионный угол также рассчитывается по одной из двух специальных методик: Нэша и Мо или Раймонди.
, с центром на Th9.")
Рентгенография грудного отдела позвоночника. Левосторонний сколиоз 2-й ст. с углом дуги около 15,8 градусов (по Коббу), с центром на Th9.
Нелучевые инструментальные методы
В периоды быстрого роста исследование позвоночника нужно проводить чаще, поэтому для снижения дозы рентгеновского облучения используются нелучевые безвредные методики, в том числе – трехмерное исследование ультразвуковым или контактным сенсором, светооптическое измерение профиля спины и сколиометрия по Буннеллю.
Возможно также выполнение снимков с малым облучением (с сокращенным временем облучения). Мелкие детали на таких снимках не просматриваются, но по ним можно проводить измерение угла искривления при сколиозе. При необходимости для выявления причины развития сколиоза может также проводиться МРТ позвоночника.

МРТ грудного отдела позвоночника. Выраженная дугообразная сколиотическая деформация грудного отдела позвоночника вправо.
Лечение сколиоза
Пациенты должны наблюдаться у опытного врача-вертебролога или ортопеда, хорошо знакомого с данной патологией. Возможное быстрое прогрессирование и воздействие искривления на состояние внутренних органов требует адекватного лечения, а также, при необходимости – направления к другим специалистам: пульмонологам, кардиологам и т. д. Лечение сколиоза может быть как консервативным, так и оперативным, в зависимости от причины и выраженности патологии, наличия или отсутствия прогрессирования. В любом случае – важно, чтобы оно было комплексным, постоянным, своевременным.
Консервативная терапия
При сколиозах, обусловленных последствиями травмы, укорочениями конечностей и другими подобными факторами необходимо в первую очередь устранить причину. Например – использовать специальные стельки или ортопедическую обувь для компенсации разницы в длине конечностей. При нейрогенных и миопатических сколиозах консервативная терапия, как правило, малоэффективна. Требуется хирургическое лечение.
Консервативное лечение идиопатических сколиозов включает в себя специальную антисколиозную гимнастику и использование корсетов. При угле искривления до 15 градусов в отсутствие ротации показана специализированная гимнастика. При угле искривления 15-20 градусов с сопутствующей ротацией (у пациентов с незавершенным ростом) к гимнастике добавляют корсетотерапию. Использование корсетов возможно как только в ночное время, так и постоянно – в зависимости от рекомендаций врача. Если рост завершился, корсет не нужен.
При прогрессирующем сколиозе с углом более 20-40 градусов показано стационарное лечение в условиях специализированной вертебрологической клиники. Если рост не завершен, рекомендуется постоянное ношение деротирующего корсета (не менее 16 часов в сутки, оптимально – 23 часа в сутки) в сочетании с интенсивной гимнастикой. После завершения роста корсет, как и в предыдущем случае, не требуется.
Хирургическое лечение
При угле более 40-45 градусов, как правило, требуется оперативное лечение. Показания к операции определяются индивидуально и зависят от причины развития сколиоза, возраста пациента, его физического и психологического состояния, вида и локализации деформации, а также эффективности консервативных методов лечения.
Операция при сколиозе представляет собой выпрямление позвоночника до определенного угла с использованием металлических конструкций. При этом подвергшийся оперативному вмешательству отдел позвоночника обездвиживается. Для фиксации позвоночника применяются специальные пластины, стержни, крючки и винты. Для расширения позвонков, придания позвоночнику более правильной формы и улучшения консолидации используются костные трансплантаты в виде вкладышей. Операция по коррекции сколиоза может проводиться трансторакально, дорсально и путем торакофренолюмботомии.
|
Литература 1. Искривление позвоночника. Сколиоз у детей и взрослых/ Амосов В.Н. — 2010 2. Травматология и ортопедия / под ред. Корнилова Н.В. — 2011 3. Заболевания и повреждения позвоночника у детей и подростков / Андрианов В.Л., Баиров Г.И., Садофьева В.И., Райе Р.Э. — 1985 4. Сколиоз и кифоз / Чаклин В.Д., Абальмасова Е.А. — 1973 |
Код МКБ-10 M41 |
Сколиоз — лечение в Москве
| Scoliosis | |
|---|---|
 |
|
| Pronunciation |
|
| Specialty | Orthopedic surgery |
| Symptoms | Sideways curve in the back[2] |
| Usual onset | 10–20 years old[2] |
| Causes | Usually unknown[3] |
| Risk factors | Family history, cerebral palsy, Marfan syndrome, tumors such as neurofibromatosis[2] |
| Diagnostic method | X-ray[2] |
| Treatment | Watchful waiting, bracing, exercises, surgery[2][4] |
| Frequency | 3%[5][6] |
Scoliosis is a condition in which a person’s spine has a sideways curve.[2] The curve is usually «S»- or «C»-shaped over three dimensions.[2][7] In some, the degree of curve is stable, while in others, it increases over time.[3] Mild scoliosis does not typically cause problems, but more severe cases can affect breathing and movement.[3][8] Pain is usually present in adults, and can worsen with age.[9]
The cause of most cases is unknown, but it is believed to involve a combination of genetic and environmental factors.[3] Risk factors include other affected family members.[2] It can also occur due to another condition such as muscle spasms, cerebral palsy, Marfan syndrome, and tumors such as neurofibromatosis.[2] Diagnosis is confirmed with X-rays.[2] Scoliosis is typically classified as either structural in which the curve is fixed, or functional in which the underlying spine is normal.[2]
Treatment depends on the degree of curve, location, and cause.[2] The age of the patient is also important, since some treatments are ineffective in adults, who are no longer growing. Minor curves may simply be watched periodically.[2] Treatments may include bracing, specific exercises, posture checking, and surgery.[2][4] The brace must be fitted to the person and used daily until growing stops.[2] Specific exercises, such as exercises that focus on the core, may be used to try to decrease the risk of worsening.[4] They may be done alone or along with other treatments such as bracing.[10][11] Evidence that chiropractic manipulation, dietary supplements, or exercises can prevent the condition from worsening is weak.[2][12] However, exercise is still recommended due to its other health benefits.[2]
Scoliosis occurs in about 3% of people.[5] It most commonly develops between the ages of ten and twenty.[2] Females typically are more severely affected than males with a ratio of 4:1.[2][3] The term is from Ancient Greek σκολίωσις (skolíōsis), which means «a bending».[13]
Signs and symptoms[edit]
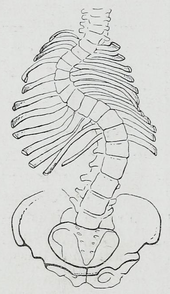
A 20th-century illustration of a severe case of an «S» shaped scoliosis
Symptoms associated with scoliosis can include:
- Pain in the back at the site of the curve, which may radiate to the legs[14]
- Respiratory or cardiac problems in severe cases[15]
- Constipation due to curvature causing «tightening» of the stomach, intestines, etc.[16]
The signs of scoliosis can include:[citation needed]
- Uneven musculature on one side of the spine[17]
- Rib prominence or a prominent shoulder blade, caused by rotation of the rib cage in thoracic scoliosis[18]
- Uneven hips, arms, or leg lengths
- Slow nerve action
- Uneven posture[18]
- Heart and lung problems in severe cases[15]
- Calcium deposits in the cartilage endplate and sometimes in the disc itself[19]
Course[edit]
People who have reached skeletal maturity are less likely to have a worsening case.[20] Some severe cases of scoliosis can lead to diminishing lung capacity, pressure exerted on the heart, and restricted physical activities.[21]
Recent longitudinal studies reveal that the most common form of the condition, late-onset idiopathic scoliosis, causes little physical impairment other than back pain and cosmetic concerns, even when untreated, with mortality rates similar to the general population.[22][23] Older beliefs that untreated idiopathic scoliosis necessarily progresses into severe (cardiopulmonary) disability by old age have been refuted by later studies.[24]
Causes[edit]
An estimated 65% of scoliosis cases are idiopathic (cause unknown), about 15% are congenital, and about 10% are secondary to a neuromuscular disease.[25]
About 38% of variance in scoliosis risk is due to genetic factors, and 62% is due to the environment.[26] The genetics are likely complex, however, given the inconsistent inheritance and discordance among monozygotic twins.[26] The specific genes that contribute to development of scoliosis have not been conclusively identified. At least one gene, CHD7, has been associated with the idiopathic form of scoliosis.[27]
Several candidate gene studies have found associations between idiopathic scoliosis and genes mediating bone formation, bone metabolism, and connective tissue structure.[26] Several genome-wide studies have identified a number of loci as significantly linked to idiopathic scoliosis.[26] In 2006, idiopathic scoliosis was linked with three microsatellite polymorphisms in the MATN1 gene (encoding for matrilin 1, cartilage matrix protein).[28] Fifty-three single nucleotide polymorphism markers in the DNA that are significantly associated with adolescent idiopathic scoliosis were identified through a genome-wide association study.[29]
Adolescent idiopathic scoliosis has no clear causal agent, and is generally believed to be multifactorial; leading to «progressive functional limitations» for individuals.[30][31][32][27][33] Research suggests that Posterior Spinal Fusion (PSF) can be used to correct the more severe deformities caused by adolescent idiopathic scoliosis.[34][35][36][37][38] Such procedures can result in a return to physical activity in about 6 months, which is very promising, although minimal back pain is still to be expected in the most severe cases.[39][40][41][42][38] The prevalence of scoliosis is 1% to 2% among adolescents, but the likelihood of progression among adolescents with a Cobb angle less than 20° is about 10% to 20%.[43]
Congenital scoliosis can be attributed to a malformation of the spine during weeks three to six in utero due to a failure of formation, a failure of segmentation, or a combination of stimuli.[44] Incomplete and abnormal segmentation results in an abnormally shaped vertebra, at times fused to a normal vertebra or unilaterally fused vertebrae, leading to the abnormal lateral curvature of the spine.[45]
Resulting from other conditions[edit]
Secondary scoliosis due to neuropathic and myopathic conditions can lead to a loss of muscular support for the spinal column so that the spinal column is pulled in abnormal directions.[citation needed] Some conditions which may cause secondary scoliosis include muscular dystrophy, spinal muscular atrophy, poliomyelitis, cerebral palsy, spinal cord trauma, and myotonia.[46][47] Scoliosis often presents itself, or worsens, during an adolescent’s growth spurt and is more often diagnosed in females than males.[43]
Scoliosis associated with known syndromes is often subclassified as «syndromic scoliosis».[48] Scoliosis can be associated with amniotic band syndrome,[49] Arnold–Chiari malformation,[50] Charcot–Marie–Tooth disease,[51] cerebral palsy,[52] congenital diaphragmatic hernia,[53] connective tissue disorders,[54] muscular dystrophy,[55] familial dysautonomia,[56] CHARGE syndrome,[57] Ehlers–Danlos syndrome[54] (hyperflexibility, «floppy baby» syndrome, and other variants of the condition), fragile X syndrome,[58][59] Friedreich’s ataxia,[60] hemihypertrophy,[61] Loeys–Dietz syndrome,[62] Marfan syndrome,[54] nail–patella syndrome,[63] neurofibromatosis,[64] osteogenesis imperfecta,[65] Prader–Willi syndrome,[66] proteus syndrome,[67] spina bifida,[68] spinal muscular atrophy,[69] syringomyelia,[70] and pectus carinatum.[71]
Another form of secondary scoliosis is degenerative scoliosis, also known as de novo scoliosis, which develops later in life secondary to degenerative (may or may not be associated with aging) changes. This is a type of deformity that starts and progresses because of the collapse of the vertebral column in an asymmetrical manner. As bones start to become weaker and the ligaments and discs located in the spine become worn as a result of age-related changes, the spine begins to curve.[72]
Diagnosis[edit]

People who initially present with scoliosis undergo a physical examination to determine whether the deformity has an underlying cause and to exclude the possibility of the underlying condition more serious than simple scoliosis.[citation needed]
The person’s gait is assessed, with an exam for signs of other abnormalities (e.g., spina bifida as evidenced by a dimple, hairy patch, lipoma, or hemangioma). A thorough neurological examination is also performed, the skin for café au lait spots, indicative of neurofibromatosis, the feet for cavovarus deformity, abdominal reflexes and muscle tone for spasticity.[citation needed]
When a person can cooperate, they are asked to bend forward as far as possible. This is known as the Adams forward bend test[73] and is often performed on school students. If a prominence is noted, then scoliosis is a possibility and an X-ray may be done to confirm the diagnosis.
As an alternative, a scoliometer may be used to diagnose the condition.[74]
When scoliosis is suspected, weight-bearing, full-spine AP/coronal (front-back view) and lateral/sagittal (side view) X-rays are usually taken to assess the scoliosis curves and the kyphosis and lordosis, as these can also be affected in individuals with scoliosis. Full-length standing spine X-rays are the standard method for evaluating the severity and progression of scoliosis, and whether it is congenital or idiopathic in nature. In growing individuals, serial radiographs are obtained at 3- to 12-month intervals to follow curve progression, and, in some instances, MRI investigation is warranted to look at the spinal cord.[75] An average scoliosis patient has been in contact with around 50-300mGy of radiation due to these radiographs during this time period.[76]
The standard method for assessing the curvature quantitatively is measuring the Cobb angle, which is the angle between two lines, drawn perpendicular to the upper endplate of the uppermost vertebra involved and the lower endplate of the lowest vertebra involved. For people with two curves, Cobb angles are followed for both curves. In some people, lateral-bending X-rays are obtained to assess the flexibility of the curves or the primary and compensatory curves.[citation needed]
Congenital and idiopathic scoliosis that develops before the age of 10 is referred to as early-onset scoliosis.[77] Progressive idiopathic early-onset scoliosis can be a life-threatening condition with negative effects on pulmonary function.[78][79] Scoliosis that develops after 10 is referred to as adolescent idiopathic scoliosis.[3] Screening adolescents without symptoms for scoliosis is of unclear benefit.[80]
Definition[edit]
Scoliosis is defined as a three-dimensional deviation in the axis of a person’s spine.[43][7] Most instances, including The Scoliosis Research Society, define scoliosis as a Cobb angle of more than 10° to the right or left as the examiner faces the person, i.e. in the coronal plane.[81]
Scoliosis has been described as a biomechanical deformity, the progression of which depends on asymmetric forces otherwise known as the Hueter-Volkmann Law.[29]
Management[edit]
Scoliosis curves do not straighten out on their own. Many children have slight curves that do not need treatment. In these cases, the children grow up to lead normal body posture by itself, even though their small curves never go away. If the patient has a larger curve and they are still growing, it is important to monitor the curve for change by periodic examination and standing x-rays as needed. The rise in spinal abnormalities require examination by an orthopaedic surgeon to determine if active treatment is needed.[82]
The traditional medical management of scoliosis is complex and is determined by the severity of the curvature and skeletal maturity, which together help predict the likelihood of progression.
The conventional options for children and adolescents are:[83]
- Observation
- Bracing
- Surgery
- Physical Therapy. Evidence suggests use of scoliosis specific exercises might prevent the progression of the curve along with possible bracing and surgery avoidance.[84]
For adults, treatment usually focuses on relieving any pain:[85][86]
- Pain medication
- Posture checking
- Bracing
- Surgery[87]
Treatment for idiopathic scoliosis also depends upon the severity of the curvature, the spine’s potential for further growth, and the risk that the curvature will progress. Mild scoliosis (less than 30° deviation) and moderate scoliosis (30–45°) can typically be treated conservatively with bracing in conjunction with scoliosis-specific exercises.[4] Severe curvatures that rapidly progress may require surgery with spinal rod placement and spinal fusion. In all cases, early intervention offers the best results.[citation needed]
A specific type of physical therapy may be useful.[88][4] Evidence to support their use however is weak.[2][12] Low quality evidence suggests scoliosis-specific exercises (SSE) may be more effective than electrostimulation.[89] Evidence for the Schroth method is insufficient to support its use.[90] Significant improvement in function, vertebral angles and trunk asymmetries have been recorded following the implementation of Schroth method in terms of conservative management of scoliosis. Some other forms of exercises interventions have been lately used in the clinical practice for therapeutic management of scoliosis such as global postural reeducation and the Klapp method.[84]
Bracing[edit]

A Chêneau brace achieving correction from 56° to 27° Cobb angle
Bracing is normally done when the person has bone growth remaining and is, in general, implemented to hold the curve and prevent it from progressing to the point where surgery is recommended. In some cases with juveniles, bracing has reduced curves significantly, going from a 40° (of the curve, mentioned in length above) out of the brace to 18°. Braces are sometimes prescribed for adults to relieve pain related to scoliosis. Bracing involves fitting the person with a device that covers the torso; in some cases, it extends to the neck (example being the Milwaukee Brace).[91]

Female adolescent (14 years old) patient wearing a Milwaukee brace — with neck ring and mandible (chin) pad showing
The most commonly used brace is a TLSO, such as a Boston brace, a corset-like an appliance that fits from armpits to hips and is custom-made from fiberglass or plastic. It is typically recommended to be worn 22–23 hours a day, and applies pressure on the curves in the spine. The effectiveness of the brace depends on not only brace design and orthotist skill, but also people’s compliance and amount of wear per day. An alternative form of brace is a nighttime only brace, that is worn only at night whilst the child sleeps, and which overcorrects the deformity.[92] Whilst nighttime braces are more convenient for children and families, it is unknown if the effectiveness of the brace is as good as conventional braces. The UK government have funded a large clinical trial (called the BASIS study) to resolve this uncertainty.[93] The BASIS study is ongoing throughout the UK in all of the leading UK children’s hospitals that treat scoliosis, with families encouraged to take part.
Indications for bracing: people who are still growing who present with Cobb angles less than 20° should be closely monitored. People who are still growing who present with Cobb angles of 20 to 29° should be braced according to the risk of progression by considering age, Cobb angle increase over a six-month period, Risser sign, and clinical presentation. People who are still growing who present with Cobb angles greater than 30° should be braced. However, these are guidelines and not every person will fit into this table.
For example, a person who is still growing with a 17° Cobb angle and significant thoracic rotation or flatback could be considered for nighttime bracing. On the opposite end of the growth spectrum, a 29° Cobb angle and a Risser sign three or four might not need to be braced because the potential for progression is reduced.[94] The Scoliosis Research Society’s recommendations for bracing include curves progressing to larger than 25°, curves presenting between 30 and 45°, Risser sign 0, 1, or 2 (an X-ray measurement of a pelvic growth area), and less than six months from the onset of menses in girls.[95]
Scoliosis braces are usually comfortable, especially when well designed and well fitted, also after the 7- to 10-day break-in period. A well fitted and functioning scoliosis brace provides comfort when it is supporting the deformity and redirecting the body into a more corrected and normal physiological position.[96]
Evidence supports that bracing prevents worsening of disease, but whether it changes quality of life, appearance, or back pain is unclear.[97]
Surgery[edit]


Preoperative (left) and postoperative (right) X-ray of a person with thoracic dextroscoliosis and lumbar levoscoliosis: The X-ray is usually projected anteroposterior, such that the right side of the subject is on the right side of the image; i.e., the subject is viewed from the rear (see left image; the right image is seen from the front). This projection is typically used by spine surgeons, as it is how surgeons see their patients when they are on the operating table (in the prone position). This is the opposite of many Chest radiographs, where the image is posteroanterior, i.e. projected as if looking at the patient from the front. The surgery was a fusion with instrumentation.[citation needed]
Surgery is usually recommended by orthopedists for curves with a high likelihood of progression (i.e., greater than 45 to 50° of magnitude), curves that would be cosmetically unacceptable as an adult, curves in people with spina bifida and cerebral palsy that interfere with sitting and care, and curves that affect physiological functions such as breathing.[98]
Surgery is indicated by the Society on Scoliosis Orthopaedic and Rehabilitation Treatment (SOSORT) at 45 to 50°[4] and by the Scoliosis Research Society (SRS) at a Cobb angle of 45°.[99] SOSORT uses the 45 to 50° threshold as a result of the well-documented, plus or minus 5° measurement error that can occur while measuring Cobb angles.[citation needed]
Surgeons who are specialized in spine surgery perform surgery for scoliosis. To completely straighten a scoliotic spine is usually impossible, but for the most part, significant corrections are achieved.[100]
The two main types of surgery are:[citation needed]
- Anterior fusion: This surgical approach is through an incision at the side of the chest wall.
- Posterior fusion: This surgical approach is through an incision on the back and involves the use of metal instrumentation to correct the curve.
One or both of these surgical procedures may be needed. The surgery may be done in one or two stages and, on average, takes four to eight hours.
A new tethering procedure (anterior vertebral body tethering) may be appropriate for some patients.
Prognosis[edit]
A 50-year follow-up study published in the Journal of the American Medical Association (2003) asserted the lifelong physical health, including cardiopulmonary and neurological functions, and mental health of people with idiopathic scoliosis are comparable to those of the general population. Scoliosis that interferes with normal systemic functions is «exceptional»[101] and «rare», and «untreated [scoliosis] people had similar death rates and were just as functional and likely to lead productive lives 50 years after diagnosis as people with normal spines.»[22][102] In an earlier University of Iowa follow-up study, 91% of people with idiopathic scoliosis displayed normal pulmonary function, and their life expectancy was found to be 2% more than that of the general population.[23] Later (2006-) studies corroborate these findings, adding that they are «reassuring for the adult patient who has adolescent onset idiopathic scoliosis in approximately the 50–70° range.»[103] These modern landmark studies supersede earlier studies (e.g. Mankin-Graham-Schauk 1964) that did implicate moderate idiopathic scoliosis in impaired pulmonary function.[citation needed]
Generally, the prognosis of scoliosis depends on the likelihood of progression. The general rules of progression are larger curves carry a higher risk of progression than smaller curves, and thoracic and double primary curves carry a higher risk of progression than single lumbar or thoracolumbar curves. In addition, people not having yet reached skeletal maturity have a higher likelihood of progression (i.e., if the person has not yet completed the adolescent growth spurt).[104]
Epidemiology[edit]
Scoliosis affects 2–3% of the United States population, which is equivalent to about five to nine million cases.[4] A scoliosis spinal column curve of 10° or less affects 1.5% to 3% of individuals.[95] The age of onset is usually between 10 years and 15 years (can occur at a younger age) in children and adolescents, making up to 85% of those diagnosed. This is seen to be due to rapid growth spurts occurring at puberty when spinal development is most relenting to genetic and environmental influences.[105] Because female adolescents undergo growth spurts before postural musculoskeletal maturity, scoliosis is more prevalent among females.[106]
Although fewer cases are present today using Cobb angle analysis for diagnosis, scoliosis remains a prevailing condition, appearing in otherwise healthy children. Despite the fact that scoliosis is a disfigurement of the spine, it has been shown to influence the pneumonic function, balance while standing and stride execution of kids with scoliosis. The impacts of backpack carriage on these three side effects have been broadly researched.[107] Incidence of idiopathic scoliosis (IS) stops after puberty when skeletal maturity is reached, however, further curvature may proceed during late adulthood due to vertebral osteoporosis and weakened musculature.[4]
History[edit]

Female with lateral curvature of the spine
Ever since the condition was discovered by the Greek physician Hippocrates, a cure has been sought. Treatments such as bracing and the insertion of rods into the spine were employed during the 1900s. In the mid-20th century, new treatments and improved screening methods have been developed to reduce the progression of scoliosis in patients and alleviate their associated pain. School children were during this period believed to develop poor posture as a result of working at their desks, and many were diagnosed with scoliosis. It was also considered to be caused by tuberculosis or poliomyelitis, diseases that were successfully managed using vaccines and antibiotics.[citation needed]
The American orthopaedic surgeon Alfred Shands Jr. discovered that two percent of patients had non-disease related scoliosis, later termed idiopathic scoliosis, or the «cancer of orthopaedic surgery». These patients were treated with questionable remedies.[108] A theory at the time—now discredited—was that the condition needed to be detected early to halt its progression, and so some schools made screening for scoliosis mandatory. Measurements of shoulder height, leg length and spinal curvature were made, and the ability to bend forwards, along with body posture, was tested, but students were sometimes misdiagnosed because of their poor posture.[citation needed]
An early treatment was the Milwaukee brace, a rigid contraption of metal rods attached to a plastic or leather girdle, designed to straighten the spine. Because of the constant pressure applied to the spine, the brace was uncomfortable. It caused jaw and muscle pain, skin irritation, as well as low self-esteem.[citation needed]
Surgery[edit]
In 1962, the American orthopaedic surgeon Paul Harrington introduced a metal spinal system of instrumentation that assisted with straightening the spine, as well as holding it rigid while fusion took place. The now obsolete Harrington rod operated on a ratchet system, attached by hooks to the spine at the top and bottom of the curvature that when cranked would distract—or straighten—the curve. The Harrington rod obviates the need for prolonged casting, allowing patients greater mobility in the postoperative period and significantly reducing the quality of life burden of fusion surgery. The Harrington rod was the precursor to most modern spinal instrumentation systems. A major shortcoming was that it failed to produce a posture wherein the skull would be in proper alignment with the pelvis, and it did not address rotational deformity. As the person aged, there would be increased wear and tear, early onset arthritis, disc degeneration, muscular stiffness, and acute pain. «Flatback» became the medical name for a related complication, especially for those who had lumbar scoliosis.[109]
In the 1960s, the gold standard for idiopathic scoliosis was a posterior approach using a single Harrington rod. Post-operative recovery involved bed rest, casts, and braces. Poor results became apparent over time.[110]
In the 1970s, an improved technique was developed using two rods and wires attached at each level of the spine. This segmented instrumentation system allowed patients to become mobile soon after surgery.[110]
In the 1980s, Cotrel-Dubousset instrumentation improved fixation and addressed sagittal imbalance and rotational defects unresolved by the Harrington rod system. This technique used multiple hooks with rods to give stronger fixation in three dimensions, usually eliminating the need for postoperative bracing.[110]
Evolution[edit]

A 14–15th-century woman who had severe scoliosis, and died at about 35 years, Limburgs Museum Venlo
There are links between human spinal morphology, bipedality, and scoliosis which suggest an evolutionary basis for the condition. Scoliosis has not been found in chimpanzees or gorillas.[111] Thus, it has been hypothesized that scoliosis may actually be related to humans’ morphological differences from these apes.[111] Other apes have a shorter and less mobile lower spine than humans. Some of the lumbar vertebrae in Pan are «captured», meaning that they are held fast between the ilium bones of the pelvis. Compared to humans, Old World monkeys have far larger erector spinae muscles, which are the muscles which hold the spine steady.[111] These factors make the lumbar spine of most primates less flexible and far less likely to deviate than those of humans. While this may explicitly relate only to lumbar scolioses, small imbalances in the lumbar spine could precipitate thoracic problems as well.[111]
Scoliosis may be a byproduct of strong selection for bipedalism. For a bipedal stance, a highly mobile, elongated lower spine is very beneficial.[111] For instance, the human spine takes on an S-shaped curve with lumbar lordosis, which allows for better balance and support of an upright trunk.[112] Selection for bipedality was likely strong enough to justify the maintenance of such a disorder. Bipedality is hypothesized to have emerged for a variety of different reasons, many of which would have certainly conferred fitness advantages. It may increase viewing distance, which can be beneficial in hunting and foraging as well as protection from predators or other humans; it makes long-distance travel more efficient for foraging or hunting; and it facilitates terrestrial feeding from grasses, trees, and bushes.[113] Given the many benefits of bipedality which depends on a particularly formed spine, it is likely that selection for bipedalism played a large role in the development of the spine as we see it today, in spite of the potential for «scoliotic deviations».[111] According to the fossil record, scoliosis may have been more prevalent among earlier hominids such as Australopithecus and Homo erectus, when bipedality was first emerging. Their fossils indicate that there may have been selected over time for a slight reduction in lumbar length to what we see today, favouring a spine that could efficiently support bipedality with a lower risk of scoliosis.[111]
Society and culture[edit]
The cost of scoliosis involves both monetary losses and lifestyle limitations that increase with severity. Respiratory deficiencies may also arise from thoracic deformities and cause abnormal breathing.[114] This directly affects exercise and work capacity, decreasing the overall quality of life.[4]
In the health care system of the United States, the average hospital cost for cases involving surgical procedures was $30,000 to $60,000 per person in 2010.[115] As of 2006, the cost of bracing has been published as up to $5,000 during rapid growth periods, when braces must be consistently replaced across multiple follow-ups.[4]
Research[edit]
Genetic testing for adolescent idiopathic scoliosis, which became available in 2009 and is still under investigation, attempts to gauge the likelihood of curve progression.[116][needs update]
See also[edit]
- Back brace
- Kyphosis
- Lordosis
- Neuromechanics of idiopathic scoliosis
- Pott disease
- Scheuermann’s disease
- Schooliosis
- Scoliosis Research Society
References[edit]
- ^ «Scoliosis». Merriam Webster. Archived from the original on 11 August 2016. Retrieved 12 August 2016.
- ^ a b c d e f g h i j k l m n o p q r s t «Questions and Answers about Scoliosis in Children and Adolescents». NIAMS. December 2015. Archived from the original on 25 August 2016. Retrieved 12 August 2016.
- ^ a b c d e f «Adolescent idiopathic scoliosis». Genetics Home Reference. September 2013. Archived from the original on 16 August 2016. Retrieved 12 August 2016.
- ^ a b c d e f g h i j Negrini S, Donzelli S, Aulisa AG, Czaprowski D, Schreiber S, de Mauroy JC, et al. (2018). «2016 SOSORT guidelines: orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth». Scoliosis and Spinal Disorders. 13: 3. doi:10.1186/s13013-017-0145-8. PMC 5795289. PMID 29435499.
- ^ a b Shakil H, Iqbal ZA, Al-Ghadir AH (2014). «Scoliosis: review of types of curves, etiological theories and conservative treatment». Journal of Back and Musculoskeletal Rehabilitation. 27 (2): 111–115. doi:10.3233/bmr-130438. PMID 24284269.
- ^ «Scoliosis — Symptoms, Diagnosis and Treatment». aans.org. Retrieved 10 February 2022.
- ^ a b Illés TS, Lavaste F, Dubousset JF (April 2019). «The third dimension of scoliosis: The forgotten axial plane». Orthopaedics & Traumatology, Surgery & Research. 105 (2): 351–359. doi:10.1016/j.otsr.2018.10.021. PMID 30665877.
- ^ Yang S, Andras LM, Redding GJ, Skaggs DL (January 2016). «Early-Onset Scoliosis: A Review of History, Current Treatment, and Future Directions». Pediatrics. 137 (1): e20150709. doi:10.1542/peds.2015-0709. PMID 26644484. S2CID 557560.
- ^ Agabegi SS, Kazemi N, Sturm PF, Mehlman CT (December 2015). «Natural History of Adolescent Idiopathic Scoliosis in Skeletally Mature Patients: A Critical Review». The Journal of the American Academy of Orthopaedic Surgeons. 23 (12): 714–723. doi:10.5435/jaaos-d-14-00037. PMID 26510624. S2CID 6735774.
- ^ Berdishevsky H, Lebel VA, Bettany-Saltikov J, Rigo M, Lebel A, Hennes A, et al. (2016). «Physiotherapy scoliosis-specific exercises — a comprehensive review of seven major schools». Scoliosis and Spinal Disorders. 11: 20. doi:10.1186/s13013-016-0076-9. PMC 4973373. PMID 27525315.
- ^ Park JH, Jeon HS, Park HW (June 2018). «Effects of the Schroth exercise on idiopathic scoliosis: a meta-analysis». European Journal of Physical and Rehabilitation Medicine. 54 (3): 440–449. doi:10.23736/S1973-9087.17.04461-6. PMID 28976171. S2CID 39497372.
- ^ a b Thompson JY, Williamson EM, Williams MA, Heine PJ, Lamb SE (June 2019). «Effectiveness of scoliosis-specific exercises for adolescent idiopathic scoliosis compared with other non-surgical interventions: a systematic review and meta-analysis». Physiotherapy. 105 (2): 214–234. doi:10.1016/j.physio.2018.10.004. PMID 30824243. S2CID 73471547.
- ^ «scoliosis». Dictionary.com Unabridged (Online). n.d. Retrieved 12 August 2016. Archived 16 August 2016 at the Wayback Machine.
- ^ Aebi, Max (2005). «The Adult Scoliosis» (PDF). European Spine Journal. 14 (10): 925–948. doi:10.1007/s00586-005-1053-9. PMID 16328223. S2CID 22119278. Retrieved 21 December 2022.
- ^ a b Nachemson, Alf (1968). «A Long Term Follow-up Study of Non-treated Scoliosis». Acta Orthopaedica Scandinavica. 39 (4): 466–476. doi:10.3109/17453676808989664. PMID 5726117. Retrieved 21 December 2022.
- ^ Yanner, Baher S. (17 December 2021). «How Scoliosis Affects the Body». spineina.com. Spine Institute of North America. Retrieved 8 January 2023.
- ^ «Muscular Imbalance: Why Does Scoliosis Create One Weak Side?». www.scoliosissos.com. Scoliosis SOS Clinic. 28 August 2017. Retrieved 10 January 2023.
- ^ a b Coillard, Christine; Leroux, Michel A.; Prince, François; Rivard, Charles H.; Zabjek, Karl Franc (2008). «Postural Characteristics of Adolescents With Idiopathic Scoliosis». Journal of Pediatric Orthopaedics. 28 (2): 218–224. doi:10.1097/BPO.0b013e3181651bdc. PMID 18388718. S2CID 34046217. Retrieved 8 January 2023.
- ^ Giachelli CM (March 1999). «Ectopic calcification: gathering hard facts about soft tissue mineralization». The American Journal of Pathology. 154 (3): 671–675. doi:10.1016/S0002-9440(10)65313-8. PMC 1866412. PMID 10079244.
- ^ Thometz JG, Simon SR (October 1988). «Progression of scoliosis after skeletal maturity in institutionalized adults who have cerebral palsy». The Journal of Bone and Joint Surgery. American Volume. 70 (9): 1290–1296. doi:10.2106/00004623-198870090-00002. PMID 3182881.
- ^ Koumbourlis AC (June 2006). «Scoliosis and the respiratory system». Paediatric Respiratory Reviews. 7 (2): 152–160. doi:10.1016/j.prrv.2006.04.009. PMID 16765303.
- ^ a b Weinstein SL, Dolan LA, Spratt KF, Peterson KK, Spoonamore MJ, Ponseti IV (February 2003). «Health and function of patients with untreated idiopathic scoliosis: a 50-year natural history study». JAMA. 289 (5): 559–567. doi:10.1001/jama.289.5.559. PMID 12578488.
- ^ a b Weinstein SL, Zavala DC, Ponseti IV (June 1981). «Idiopathic scoliosis: long-term follow-up and prognosis in untreated patients». The Journal of Bone and Joint Surgery. American Volume. 63 (5): 702–712. doi:10.2106/00004623-198163050-00003. PMID 6453874. S2CID 22429772.
- ^ Trobisch P, Suess O, Schwab F (December 2010). «Idiopathic scoliosis». Deutsches Ärzteblatt International. 107 (49): 875–83, quiz 884. doi:10.3238/arztebl.2010.0875. PMC 3011182. PMID 21191550.
It was once assumed, on the basis of studies in heterogeneous patient populations, that patients with untreated adolescent scoliosis would necessarily become wheelchair-dependent in old age and were likely to die of cardiopulmonary arrest for reasons related to scoliosis. This is no longer held to be the case.
- ^ Agabegi ED, Agabegi SS (2008). Step-Up to Medicine. Step-Up Series. Hagerstwon, MD: Lippincott Williams & Wilkins. p. 90. ISBN 978-0-7817-7153-5.
- ^ a b c d Gorman KF, Julien C, Moreau A (October 2012). «The genetic epidemiology of idiopathic scoliosis». European Spine Journal. 21 (10): 1905–1919. doi:10.1007/s00586-012-2389-6. PMC 3463687. PMID 22695700.
- ^ a b Ogilvie JW, Braun J, Argyle V, Nelson L, Meade M, Ward K (March 2006). «The search for idiopathic scoliosis genes». Spine. 31 (6): 679–681. doi:10.1097/01.brs.0000202527.25356.90. PMID 16540873. S2CID 24280322.
- ^ Montanaro L, Parisini P, Greggi T, Di Silvestre M, Campoccia D, Rizzi S, Arciola CR (December 2006). «Evidence of a linkage between matrilin-1 gene (MATN1) and idiopathic scoliosis». Scoliosis. 1: 21. doi:10.1186/1748-7161-1-21. PMC 1769398. PMID 17176459.
- ^ a b Ogilvie J (February 2010). «Adolescent idiopathic scoliosis and genetic testing». Current Opinion in Pediatrics. 22 (1): 67–70. doi:10.1097/MOP.0b013e32833419ac. PMID 19949338. S2CID 1044562.
- ^ Cheng JC, Castelein RM, Chu WC, Danielsson AJ, Dobbs MB, Grivas TB, et al. (September 2015). «Adolescent idiopathic scoliosis». Nature Reviews. Disease Primers. 1: 15030. doi:10.1038/nrdp.2015.30. PMID 27188385. S2CID 21284193.
- ^ Burwell RG (2003). «Aetiology of idiopathic scoliosis: current concepts». Pediatric Rehabilitation. 6 (3–4): 137–170. doi:10.1080/13638490310001642757. PMID 14713582. S2CID 12154979.
- ^ Shahidi B, Yoo A, Farnsworth C, Newton PO, Ward SR (September 2021). «Paraspinal muscle morphology and composition in adolescent idiopathic scoliosis: A histological analysis». JOR Spine. 4 (3): e1169. doi:10.1002/jsp2.1169. PMC 8479518. PMID 34611591.
- ^ Kouwenhoven JW, Castelein RM (December 2008). «The pathogenesis of adolescent idiopathic scoliosis: review of the literature». Spine. 33 (26): 2898–2908. doi:10.1097/BRS.0b013e3181891751. PMID 19092622. S2CID 19749217.
- ^ Weiss HR, Goodall D (August 2008). «Rate of complications in scoliosis surgery — a systematic review of the Pub Med literature». Scoliosis. 3: 9. doi:10.1186/1748-7161-3-9. PMC 2525632. PMID 18681956.
- ^ Fischer CR, Kim Y (July 2011). «Selective fusion for adolescent idiopathic scoliosis: a review of current operative strategy». European Spine Journal. 20 (7): 1048–1057. doi:10.1007/s00586-011-1730-9. PMC 3176697. PMID 21387194.
- ^ Merola AA, Haher TR, Brkaric M, Panagopoulos G, Mathur S, Kohani O, et al. (September 2002). «A multicenter study of the outcomes of the surgical treatment of adolescent idiopathic scoliosis using the Scoliosis Research Society (SRS) outcome instrument». Spine. 27 (18): 2046–2051. doi:10.1097/00007632-200209150-00015. PMID 12634567.
- ^ Chen Z, Rong L (February 2016). «Comparison of combined anterior-posterior approach versus posterior-only approach in treating adolescent idiopathic scoliosis: a meta-analysis». European Spine Journal. 25 (2): 363–371. doi:10.1007/s00586-015-3968-0. PMID 25900299. S2CID 4434949.
- ^ a b Rapp van Roden EA, Richardson RT, Russo SA, Rose WC, Nicholson KF, Chafetz RS, et al. (January 2019). «Analysis of Shoulder Complex Function After Posterior Spinal Fusion in Adolescents With Idiopathic Scoliosis». Journal of Pediatric Orthopedics. 39 (1): e32–e38. doi:10.1097/BPO.0000000000001267. PMID 30312252. S2CID 52975845.
- ^ Bastrom TP, Marks MC, Yaszay B, Newton PO, et al. (Harms Study Group) (October 2013). «Prevalence of postoperative pain in adolescent idiopathic scoliosis and the association with preoperative pain». Spine. 38 (21): 1848–1852. doi:10.1097/brs.0b013e3182a4aa97. PMID 23883827.
- ^ Landman Z, Oswald T, Sanders J, Diab M, et al. (Spinal Deformity Study Group) (May 2011). «Prevalence and predictors of pain in surgical treatment of adolescent idiopathic scoliosis». Spine. 36 (10): 825–829. doi:10.1097/brs.0b013e3181de8c2b. PMID 21192302. S2CID 205514923.
- ^ Rubery PT, Bradford DS (February 2002). «Athletic activity after spine surgery in children and adolescents: results of a survey». Spine. 27 (4): 423–427. doi:10.1097/00007632-200202150-00019. PMID 11840110. S2CID 19524978.
- ^ Tarrant RC, O’Loughlin PF, Lynch S, Queally JM, Sheeran P, Moore DP, Kiely PJ (August 2014). «Timing and predictors of return to short-term functional activity in adolescent idiopathic scoliosis after posterior spinal fusion: a prospective study». Spine. 39 (18): 1471–1478. doi:10.1097/brs.0000000000000452. PMID 24875955. S2CID 35816768.
- ^ a b c Trobisch P, Suess O, Schwab F (December 2010). «Idiopathic scoliosis». Deutsches Ärzteblatt International. 107 (49): 875–83, quiz 884. doi:10.3238/arztebl.2010.0875. PMC 3011182. PMID 21191550.
- ^ «What is Scoliosis: What Causes Scoliosis?». MedicalBug. 17 February 2012. Archived from the original on 9 April 2012. Retrieved 18 March 2012.
- ^ Scoliosis Research Society. (2014). Congenital Scoliosis. Scoliosis Research Society. «Congenital Scoliosis — Scoliosis Research Society (SRS)». Archived from the original on 1 July 2014. Retrieved 21 May 2014.
- ^ Trontelj JV, Pecak F, Dimitrijević MR (August 1979). «Segmental neurophysiological mechanisms in scoliosis». The Journal of Bone and Joint Surgery. British Volume. 61-B (3): 310–313. doi:10.1302/0301-620x.61b3.479254. PMID 479254.
- ^ POSNA. (2014). Neuromuscular Scoliosis. The Pediatric Orthopaedic Society of North America. «Neuromuscular Scoliosis — POSNA». Archived from the original on 21 May 2014. Retrieved 21 May 2014.
- ^ Chung AS, Renfree S, Lockwood DB, Karlen J, Belthur M (November 2019). «Syndromic Scoliosis: National Trends in Surgical Management and Inpatient Hospital Outcomes: A 12-Year Analysis». Spine. 44 (22): 1564–1570. doi:10.1097/BRS.0000000000003134. PMID 31689252. S2CID 201175687.
- ^ Komazec, Jovan; Matic, Aleksandra (2009). «Amniotic Band Syndrome» (PDF). Acta Medica Medianae. 48 (2): 44–48. Retrieved 29 January 2023.
- ^ «Chiari malformation». mayoclinic.org. Mayo Clinic. Retrieved 29 January 2023.
- ^ Marchesi, Chiara; Pareyson, Davide (2009). «Diagnosis, natural history, and management of Charcot-Marie-Tooth disease» (PDF). The Lancet Neurology. 8 (7): 654–667. doi:10.1016/S1474-4422(09)70110-3. PMID 19539237. S2CID 665324. Retrieved 29 January 2023.
- ^ Krigger, Karen W. (2006). «Celebral Palsy: An Overview». American Family Physician. 73 (1): 91–100. PMID 16417071. Retrieved 29 January 2023.
- ^ Chandraekharan, Praveen Kumar; Lakshminrusimha, Satyan; Madappa, Rajeshwari; Rawat, Munmun; Rothstein, David H. (2017). «Congenital Diaphragmatic hernia — a review». Maternal Health, Neonatology and Perinatology. 3: 6. doi:10.1186/s40748-017-0045-1. PMC 5356475. PMID 28331629.
- ^ a b c Hresko, M. Timothy (2013). «Idiopathic Scoliosis in Adolescents» (PDF). The New England Journal of Medicine. 368 (9): 834–841. doi:10.1056/NEJMcp1209063. PMID 23445094. Retrieved 29 January 2023.
- ^ Aartsma-Ra, Annemieke; Duan, Dongsheng; Goemans, Nathalie; Mercuri, Eugenio; Takeda, Shin’ichi (2021). «Duchenne muscular dystrophy». Nature Reviews Disease Primers. 7.
- ^ Fuente-Mora, Cristina; Kauffman, Horacio; Mendoza-Santiesteban, Carlos; Norcliffe-Kauffman, Lucy; Palma, Jose-Alberto; Percival, Leila (2014). «Current treatments in familial dysautonomia». Expert Opinion on Pharmacotherapy. 15 (18): 2653–2671. doi:10.1517/14656566.2014.970530. PMC 4236240. PMID 25323828. Retrieved 29 January 2023.
- ^ Blake, Kim D; Prasad, Chitra (2006). «CHARGE syndrome». Orphanet Journal of Rare Diseases. 1: 34. doi:10.1186/1750-1172-1-34. PMC 1586184. PMID 16959034.
- ^ «Fragile X syndrome». Department for Work and Pensions, UK. Archived from the original on 19 March 2012. Retrieved 29 August 2011.
- ^ Davids JR, Hagerman RJ, Eilert RE (July 1990). «Orthopaedic aspects of fragile-X syndrome». The Journal of Bone and Joint Surgery. American Volume. 72 (6): 889–896. doi:10.2106/00004623-199072060-00015. PMID 2195034.
- ^ Delatycki, Martin B; Forrest, Susan M; Williamson, Robert (2000). «Freidreich ataxia: an overview» (PDF). Journal of Medical Genetics. 37 (1): 1–8. doi:10.1136/jmg.37.1.1. PMC 1734457. PMID 10633128. Retrieved 30 January 2023.
- ^ Sheth, Ujash (2021). «Hemihypertrophy». www.orthobullets.com. OrthoBullets. Retrieved 31 January 2023.
- ^ Black, James H.; Bowdin, Sarah; Dietz, Harry C.; El-Hamamsy, Ismail; Frischmeyer-Guerrerio, Pamela A.; Guerrerio, Anthony L.; Loeys, Bart; MacCarrick, Gretchen; Sponseller, Paul D (2014). «Loeys-Dietz syndrome: a primer for diagnosis and management». Genetics in Medicine. 16 (8): 576–587. doi:10.1038/gim.2014.11. PMC 4131122. PMID 24577266.
- ^ Fryer, G; Green, A; McIntosh, I; Mountford, R; Sweeney, E (2003). «Nail patella syndrome: a review of the phenotype aided by developmental biology» (PDF). Journal of Medical Genetics. 40 (3): 153–162. doi:10.1136/jmg.40.3.153. PMC 1735400. PMID 12624132. Retrieved 30 January 2023.
- ^ Boyd, Kevin P.; Korf, Bruce R.; Theos, Amy (2009). «Neurofibromatosis type 1». Journal of the American Academy of Dermatology. 61 (1): 1–16. doi:10.1016/j.jaad.2008.12.051. PMC 2716546. PMID 19539839.
- ^ Glorieux, Francis H; Rauch, Frank (2004). «Osteogenesis imperfecta» (PDF). The Lancet. 363 (9418): 1377–1385. doi:10.1016/S0140-6736(04)16051-0. PMID 15110498. S2CID 24081895. Retrieved 30 January 2023.
- ^ Cassidy, Suzanne B.; Driscoll, Daniel J.; Miller, Jennifer L.; Schwartz, Stuart (2012). «Prader-Willi syndrome». Genetics in Medicine. 14 (1): 10–26. doi:10.1038/gim.0b013e31822bead0. PMID 22237428. S2CID 19992. Retrieved 30 January 2023.
- ^ Biesecker, Leslie G.; Choyke, Peter L.; Jamis-Dow, Carlos A.; Turner, Joyce (2004). «Radiologic Manifestations of Proteus Syndrome» (PDF). RadioGraphics. 24 (4): 1051–1068. doi:10.1148/rg.244035726. PMID 15256628. Retrieved 31 January 2023.
- ^ Adzick, N Scott; Melchionne, Jeanne; Mitchell, Laura E; Pasquariello, Patrick S; Sutton, Leslie N; Whitehead, Alexander S (2004). «Spina bifida». The Lancet. 364 (9448): 1885–1895. doi:10.1016/S0140-6736(04)17445-X. PMID 15555669. S2CID 37770338. Retrieved 31 January 2023.
- ^ Lunn, Mitchell R; Wang, Ching H (2008). «Spinal muscular atrophy». The Lancet. 371 (9630): 2120–2133. doi:10.1016/S0140-6736(08)60921-6. PMID 18572081. S2CID 11023418. Retrieved 31 January 2023.
- ^ Vandertop, W. Peter (2014). «Syringomyelia». Neuropediatrics. 45 (1): 003–009. doi:10.1055/s-0033-1361921. PMID 24272770. Retrieved 31 January 2023.
- ^ Desmarais, Thomas J.; Keller, Martin S. (2013). «Pectus carinatum» (PDF). Current Opinion in Pediatrics. 25 (3): 375–381. doi:10.1097/MOP.0b013e3283604088. PMID 23657247. S2CID 46604820. Retrieved 31 January 2023.
- ^ Giradi, Federico; Hughes, Alex; Kotwal, Suhel; Pumberger, Matthias (2011). «Degenerative Scoliosis: A Review». HSS Journal. 7 (3): 257–264. doi:10.1007/s11420-011-9204-5. PMC 3192887. PMID 23024623.
- ^ «Scoliosis symptoms – pain, flat back, screening, self-assessment». iscoliosis.com.
- ^ «Scoliometer (Inclinometer)». National Scoliosis Foundation. Archived from the original on 21 November 2014.
- ^ Kim H, Kim HS, Moon ES, Yoon CS, Chung TS, Song HT, et al. (November 2010). «Scoliosis imaging: what radiologists should know». Radiographics. 30 (7): 1823–1842. doi:10.1148/rg.307105061. PMID 21057122.
The main purpose of performing CT or MR imaging in a patient with scoliosis is to identify an underlying cause. MR imaging is used with increasing frequency to evaluate patients with an unusual curve pattern or alarming clinical manifestations. Nevertheless, two reasons for performing such screening are plausible: First, the treatment of an underlying neurologic lesion could help alleviate progressive neurologic deterioration and lead to improvement or stabilization of scoliosis; second, surgery performed to correct scoliosis in the presence of an underlying neurologic disorder that has not been identified and treated could result in new or additional neurologic deficits.
- ^ Oakley PA, Ehsani NN, Harrison DE (1 April 2019). «The Scoliosis Quandary: Are Radiation Exposures From Repeated X-Rays Harmful?». Dose-Response. 17 (2): 1559325819852810. doi:10.1177/1559325819852810. PMC 6560808. PMID 31217755.
- ^ «Early Onset Scoliosis | Scoliosis Research Society». www.srs.org. Archived from the original on 21 June 2016. Retrieved 10 July 2016.
- ^ Sponseller PD, Yazici M, Demetracopoulos C, et al. Evidence basisfor management of spine and chest wall deformities in children.Spine(Phila Pa 1976). 2007;32(suppl):S81–S90
- ^ Celebioglu E., Yataganbaba A., Bekmez S., et al Growing-rod Graduates with Idiopathic Early-onset Scoliosis Have Comparable Exercise Tolerance to Patients with Surgically Treated Adolescent Idiopathic Scoliosis. J. Pediatr. Orthop.. 2020;40(8):e734-e739. doi:10.1097/BPO.0000000000001567
- ^ Grossman DC, Curry SJ, Owens DK, Barry MJ, Davidson KW, Doubeni CA, et al. (January 2018). «Screening for Adolescent Idiopathic Scoliosis: US Preventive Services Task Force Recommendation Statement». JAMA. 319 (2): 165–172. doi:10.1001/jama.2017.19342. PMID 29318284. S2CID 38852032.
- ^ Lau K. The Complete Scoliosis Surgery Handbook for Patients: An In-Depth and Unbiased Look Into What to Expect Before and During Scoliosis Surgery. Health In Your Hands. p. 89. ISBN 978-9810785925.
- ^ «Treatment Options | Scoliosis Research Society». www.srs.org. Retrieved 11 February 2022.
- ^ «Treating scoliosis in children». NHS Choices. 19 February 2013. Archived from the original on 14 May 2014. Retrieved 14 May 2014.
- ^ a b Ceballos Laita L, Tejedor Cubillo C, Mingo Gómez T, Jiménez Del Barrio S (August 2018). «Effects of corrective, therapeutic exercise techniques on adolescent idiopathic scoliosis. A systematic review». Archivos Argentinos de Pediatria. 116 (4): e582–e589. doi:10.5546/aap.2018.eng.e582. PMID 30016036.
- ^ «Scoliosis – Treatment in adults». NHS Choices. 19 February 2013. Archived from the original on 14 May 2014. Retrieved 14 May 2014.
- ^ «Idiopathic Scoliosis – Adult Nonoperative Management». Scoliosis Research Society. Archived from the original on 1 July 2014. Retrieved 14 May 2014.
- ^ «Idiopathic Scoliosis – Adult Surgical Treatment». Scoliosis Research Society. Archived from the original on 1 July 2014. Retrieved 14 May 2014.
- ^ Negrini S, Fusco C, Minozzi S, Atanasio S, Zaina F, Romano M (2008). «Exercises reduce the progression rate of adolescent idiopathic scoliosis: results of a comprehensive systematic review of the literature». Disability and Rehabilitation. 30 (10): 772–785. doi:10.1080/09638280801889568. PMID 18432435. S2CID 13188152.
- ^ Romano M, Minozzi S, Bettany-Saltikov J, Zaina F, Chockalingam N, Kotwicki T, et al. (August 2012). «Exercises for adolescent idiopathic scoliosis». The Cochrane Database of Systematic Reviews. 2012 (8): CD007837. doi:10.1002/14651858.cd007837.pub2. PMC 7386883. PMID 22895967.
- ^ Day JM, Fletcher J, Coghlan M, Ravine T (2019). «Review of scoliosis-specific exercise methods used to correct adolescent idiopathic scoliosis». Archives of Physiotherapy. 9: 8. doi:10.1186/s40945-019-0060-9. PMC 6708126. PMID 31463082.
- ^ The influence of elastic orthotic belt on sagittal profile in adolescent idiopathic thoracic scoliosis: A comparative radiographic study with Milwaukee brace., Research Gate, September 2010
- ^ Antoine L, Nathan D, Laure M, Briac C, Jean-François M, Corinne B (March 2020). «Compliance with night-time overcorrection bracing in adolescent idiopathic scoliosis: Result from a cohort follow-up». Medical Engineering & Physics. 77: 137–141. doi:10.1016/j.medengphy.2020.01.003. PMID 31992499. S2CID 210945485.
- ^ «BASIS study».
- ^ Wood G (2013). «To Brace or Not to Brace: The Three-Dimensional Nature and Growth Considerations for Adolescent Idiopathic Scoliosis». Academy Today (The Edge). American Academy of Orthosits and Prosthetist. pp. 5–8.
- ^ a b Herring JA (2002). Tachdjian’s Pediatric Orthopaedics. Philadelphia, PA: W.B. Saunders. ISBN 978-0-7216-5684-7.[page needed]
- ^ Wood GI (2013). The Cheneau Brace using Rigo Principles and the Wood Cheneau Rigo (WCR) Brace. Society on Scoliosis Orthopaedic and Rehabilitation Treatment (SOSORT). Chicago, IL.
- ^ Negrini S, Minozzi S, Bettany-Saltikov J, Chockalingam N, Grivas TB, Kotwicki T, et al. (June 2015). «Braces for idiopathic scoliosis in adolescents». The Cochrane Database of Systematic Reviews (6): CD006850. doi:10.1002/14651858.CD006850.pub3. hdl:2434/721317. PMID 26086959.
- ^ Alli RA (19 December 2020). «Scoliosis Treatment». WebMD. Retrieved 11 February 2020.
- ^ «Adolescent Idiopathic Scoliosis — Scoliosis Research Society (SRS)». Archived from the original on 16 January 2014. Retrieved 2 January 2014. adolescents/surgical_treatment.htm. Accessed 27 January 2013
- ^ Gibson I, Jagdish BN, Zhan G, Hajizedah K, Tho HK, Mengjie H, Dissanayake C (January 2012). «Development of a human spine simulation system.». In Yu W, Chattopadhyay S, Lim TC, Acharya UR (eds.). Advances in Therapeutic Engineering. CRC Press. p. 27. ISBN 978-1-4398-7174-4.
- ^ Hawes MC (May 2003). «Health and Function of Patients With Untreated Idiopathic Scoliosis—Reply». JAMA. 289 (20): 2644, author reply 2644–5. doi:10.1001/jama.289.20.2644-a. PMID 12771105.
- ^ «Many With Scoliosis Can Skip Treatments». stopgettingsick.com. Archived from the original on 20 August 2008.
- ^ Asher MA, Burton DC (March 2006). «Adolescent idiopathic scoliosis: natural history and long term treatment effects». Scoliosis. 1 (1): 2. doi:10.1186/1748-7161-1-2. PMC 1475645. PMID 16759428. S2CID 14194273.
- ^ «Adolescent Idiopathic Scoliosis | Scoliosis Research Society». www.srs.org. Retrieved 28 February 2018.
- ^ Edery P, Margaritte-Jeannin P, Biot B, Labalme A, Bernard JC, Chastang J, et al. (August 2011). «New disease gene location and high genetic heterogeneity in idiopathic scoliosis». European Journal of Human Genetics. 19 (8): 865–869. doi:10.1038/ejhg.2011.31. PMC 3172921. PMID 21407261.
- ^ Burwell RG (2003). «Aetiology of idiopathic scoliosis: current concepts». Pediatric Rehabilitation. 6 (3–4): 137–70. doi:10.1080/13638490310001642757. PMID 14713582. S2CID 12154979.
- ^ Bessette A, Rousseau CM, eds. (October 2012). Scoliosis : Causes, Symptoms and Treatment. Nova Science Publishers. ISBN 978-1-62081-007-1.
- ^ Linker B (April 2012). «A dangerous curve: the role of history in America’s scoliosis screening programs». American Journal of Public Health. 102 (4): 606–616. doi:10.2105/AJPH.2011.300531. PMC 3489358. PMID 22397340.
- ^ «Scoliosis Surgery». News-medical.net. 22 November 2009. Retrieved 16 January 2011.
- ^ a b c Bridwell K (8 February 2013). «Idiopathic Scoliosis: Options of Fixation and Fusion of Thoracic Curves». SpineUniverse. Retrieved 21 May 2014.
- ^ a b c d e f g Lovejoy CO (January 2005). «The natural history of human gait and posture. Part 1. Spine and pelvis». Gait & Posture. 21 (1): 95–112. doi:10.1016/s0966-6362(04)00014-1. PMID 15536039.
- ^ Harcourt-Smith WE (2007). «Chapter 5». Handbook of Paleoanthropology. Springer Berlin Heidelberg. pp. 1483–1518.
- ^ Hunt KD (March 1994). «The evolution of human bipedality: ecology and functional morphology». Journal of Human Evolution. 26 (3): 182–202. doi:10.1006/jhev.1994.1011.
- ^ Larson N (August 2011). «Early onset scoliosis: what the primary care provider needs to know and implications for practice». Journal of the American Academy of Nurse Practitioners. 23 (8): 392–403. doi:10.1111/j.1745-7599.2011.00634.x. PMID 21790832. S2CID 25902637.
- ^ Kamerlink JR, Quirno M, Auerbach JD, Milby AH, Windsor L, Dean L, et al. (May 2010). «Hospital cost analysis of adolescent idiopathic scoliosis correction surgery in 125 consecutive cases». The Journal of Bone and Joint Surgery. American Volume. 92 (5): 1097–1104. doi:10.2106/JBJS.I.00879. PMID 20439654.
- ^ Stenning M, Nelson I (2011). «Recent advances in the treatment of scoliosis in children». British Editorial Society of Bone and Joint Surgery. Archived from the original on 2 January 2014. Retrieved 1 January 2014.
External links[edit]
![]()
Wikimedia Commons has media related to Scoliosis.
- Scoliosis at Curlie
- Early Onset Scoliosis is the abnormal, side-to-side curve of the spine in children under five years old, often including children with congenital scoliosis (present at birth, with spine abnormalities) and infantile scoliosis (birth to three years).
- Questions and Answers about Scoliosis in Children and Adolescents – US National Institute of Arthritis and Musculoskeletal and Skin Diseases
| Scoliosis | |
|---|---|
|
|
| Pronunciation |
|
| Specialty | Orthopedic surgery |
| Symptoms | Sideways curve in the back[2] |
| Usual onset | 10–20 years old[2] |
| Causes | Usually unknown[3] |
| Risk factors | Family history, cerebral palsy, Marfan syndrome, tumors such as neurofibromatosis[2] |
| Diagnostic method | X-ray[2] |
| Treatment | Watchful waiting, bracing, exercises, surgery[2][4] |
| Frequency | 3%[5][6] |
Scoliosis is a condition in which a person’s spine has a sideways curve.[2] The curve is usually «S»- or «C»-shaped over three dimensions.[2][7] In some, the degree of curve is stable, while in others, it increases over time.[3] Mild scoliosis does not typically cause problems, but more severe cases can affect breathing and movement.[3][8] Pain is usually present in adults, and can worsen with age.[9]
The cause of most cases is unknown, but it is believed to involve a combination of genetic and environmental factors.[3] Risk factors include other affected family members.[2] It can also occur due to another condition such as muscle spasms, cerebral palsy, Marfan syndrome, and tumors such as neurofibromatosis.[2] Diagnosis is confirmed with X-rays.[2] Scoliosis is typically classified as either structural in which the curve is fixed, or functional in which the underlying spine is normal.[2]
Treatment depends on the degree of curve, location, and cause.[2] The age of the patient is also important, since some treatments are ineffective in adults, who are no longer growing. Minor curves may simply be watched periodically.[2] Treatments may include bracing, specific exercises, posture checking, and surgery.[2][4] The brace must be fitted to the person and used daily until growing stops.[2] Specific exercises, such as exercises that focus on the core, may be used to try to decrease the risk of worsening.[4] They may be done alone or along with other treatments such as bracing.[10][11] Evidence that chiropractic manipulation, dietary supplements, or exercises can prevent the condition from worsening is weak.[2][12] However, exercise is still recommended due to its other health benefits.[2]
Scoliosis occurs in about 3% of people.[5] It most commonly develops between the ages of ten and twenty.[2] Females typically are more severely affected than males with a ratio of 4:1.[2][3] The term is from Ancient Greek σκολίωσις (skolíōsis), which means «a bending».[13]
Signs and symptoms[edit]
A 20th-century illustration of a severe case of an «S» shaped scoliosis
Symptoms associated with scoliosis can include:
- Pain in the back at the site of the curve, which may radiate to the legs[14]
- Respiratory or cardiac problems in severe cases[15]
- Constipation due to curvature causing «tightening» of the stomach, intestines, etc.[16]
The signs of scoliosis can include:[citation needed]
- Uneven musculature on one side of the spine[17]
- Rib prominence or a prominent shoulder blade, caused by rotation of the rib cage in thoracic scoliosis[18]
- Uneven hips, arms, or leg lengths
- Slow nerve action
- Uneven posture[18]
- Heart and lung problems in severe cases[15]
- Calcium deposits in the cartilage endplate and sometimes in the disc itself[19]
Course[edit]
People who have reached skeletal maturity are less likely to have a worsening case.[20] Some severe cases of scoliosis can lead to diminishing lung capacity, pressure exerted on the heart, and restricted physical activities.[21]
Recent longitudinal studies reveal that the most common form of the condition, late-onset idiopathic scoliosis, causes little physical impairment other than back pain and cosmetic concerns, even when untreated, with mortality rates similar to the general population.[22][23] Older beliefs that untreated idiopathic scoliosis necessarily progresses into severe (cardiopulmonary) disability by old age have been refuted by later studies.[24]
Causes[edit]
An estimated 65% of scoliosis cases are idiopathic (cause unknown), about 15% are congenital, and about 10% are secondary to a neuromuscular disease.[25]
About 38% of variance in scoliosis risk is due to genetic factors, and 62% is due to the environment.[26] The genetics are likely complex, however, given the inconsistent inheritance and discordance among monozygotic twins.[26] The specific genes that contribute to development of scoliosis have not been conclusively identified. At least one gene, CHD7, has been associated with the idiopathic form of scoliosis.[27]
Several candidate gene studies have found associations between idiopathic scoliosis and genes mediating bone formation, bone metabolism, and connective tissue structure.[26] Several genome-wide studies have identified a number of loci as significantly linked to idiopathic scoliosis.[26] In 2006, idiopathic scoliosis was linked with three microsatellite polymorphisms in the MATN1 gene (encoding for matrilin 1, cartilage matrix protein).[28] Fifty-three single nucleotide polymorphism markers in the DNA that are significantly associated with adolescent idiopathic scoliosis were identified through a genome-wide association study.[29]
Adolescent idiopathic scoliosis has no clear causal agent, and is generally believed to be multifactorial; leading to «progressive functional limitations» for individuals.[30][31][32][27][33] Research suggests that Posterior Spinal Fusion (PSF) can be used to correct the more severe deformities caused by adolescent idiopathic scoliosis.[34][35][36][37][38] Such procedures can result in a return to physical activity in about 6 months, which is very promising, although minimal back pain is still to be expected in the most severe cases.[39][40][41][42][38] The prevalence of scoliosis is 1% to 2% among adolescents, but the likelihood of progression among adolescents with a Cobb angle less than 20° is about 10% to 20%.[43]
Congenital scoliosis can be attributed to a malformation of the spine during weeks three to six in utero due to a failure of formation, a failure of segmentation, or a combination of stimuli.[44] Incomplete and abnormal segmentation results in an abnormally shaped vertebra, at times fused to a normal vertebra or unilaterally fused vertebrae, leading to the abnormal lateral curvature of the spine.[45]
Resulting from other conditions[edit]
Secondary scoliosis due to neuropathic and myopathic conditions can lead to a loss of muscular support for the spinal column so that the spinal column is pulled in abnormal directions.[citation needed] Some conditions which may cause secondary scoliosis include muscular dystrophy, spinal muscular atrophy, poliomyelitis, cerebral palsy, spinal cord trauma, and myotonia.[46][47] Scoliosis often presents itself, or worsens, during an adolescent’s growth spurt and is more often diagnosed in females than males.[43]
Scoliosis associated with known syndromes is often subclassified as «syndromic scoliosis».[48] Scoliosis can be associated with amniotic band syndrome,[49] Arnold–Chiari malformation,[50] Charcot–Marie–Tooth disease,[51] cerebral palsy,[52] congenital diaphragmatic hernia,[53] connective tissue disorders,[54] muscular dystrophy,[55] familial dysautonomia,[56] CHARGE syndrome,[57] Ehlers–Danlos syndrome[54] (hyperflexibility, «floppy baby» syndrome, and other variants of the condition), fragile X syndrome,[58][59] Friedreich’s ataxia,[60] hemihypertrophy,[61] Loeys–Dietz syndrome,[62] Marfan syndrome,[54] nail–patella syndrome,[63] neurofibromatosis,[64] osteogenesis imperfecta,[65] Prader–Willi syndrome,[66] proteus syndrome,[67] spina bifida,[68] spinal muscular atrophy,[69] syringomyelia,[70] and pectus carinatum.[71]
Another form of secondary scoliosis is degenerative scoliosis, also known as de novo scoliosis, which develops later in life secondary to degenerative (may or may not be associated with aging) changes. This is a type of deformity that starts and progresses because of the collapse of the vertebral column in an asymmetrical manner. As bones start to become weaker and the ligaments and discs located in the spine become worn as a result of age-related changes, the spine begins to curve.[72]
Diagnosis[edit]
People who initially present with scoliosis undergo a physical examination to determine whether the deformity has an underlying cause and to exclude the possibility of the underlying condition more serious than simple scoliosis.[citation needed]
The person’s gait is assessed, with an exam for signs of other abnormalities (e.g., spina bifida as evidenced by a dimple, hairy patch, lipoma, or hemangioma). A thorough neurological examination is also performed, the skin for café au lait spots, indicative of neurofibromatosis, the feet for cavovarus deformity, abdominal reflexes and muscle tone for spasticity.[citation needed]
When a person can cooperate, they are asked to bend forward as far as possible. This is known as the Adams forward bend test[73] and is often performed on school students. If a prominence is noted, then scoliosis is a possibility and an X-ray may be done to confirm the diagnosis.
As an alternative, a scoliometer may be used to diagnose the condition.[74]
When scoliosis is suspected, weight-bearing, full-spine AP/coronal (front-back view) and lateral/sagittal (side view) X-rays are usually taken to assess the scoliosis curves and the kyphosis and lordosis, as these can also be affected in individuals with scoliosis. Full-length standing spine X-rays are the standard method for evaluating the severity and progression of scoliosis, and whether it is congenital or idiopathic in nature. In growing individuals, serial radiographs are obtained at 3- to 12-month intervals to follow curve progression, and, in some instances, MRI investigation is warranted to look at the spinal cord.[75] An average scoliosis patient has been in contact with around 50-300mGy of radiation due to these radiographs during this time period.[76]
The standard method for assessing the curvature quantitatively is measuring the Cobb angle, which is the angle between two lines, drawn perpendicular to the upper endplate of the uppermost vertebra involved and the lower endplate of the lowest vertebra involved. For people with two curves, Cobb angles are followed for both curves. In some people, lateral-bending X-rays are obtained to assess the flexibility of the curves or the primary and compensatory curves.[citation needed]
Congenital and idiopathic scoliosis that develops before the age of 10 is referred to as early-onset scoliosis.[77] Progressive idiopathic early-onset scoliosis can be a life-threatening condition with negative effects on pulmonary function.[78][79] Scoliosis that develops after 10 is referred to as adolescent idiopathic scoliosis.[3] Screening adolescents without symptoms for scoliosis is of unclear benefit.[80]
Definition[edit]
Scoliosis is defined as a three-dimensional deviation in the axis of a person’s spine.[43][7] Most instances, including The Scoliosis Research Society, define scoliosis as a Cobb angle of more than 10° to the right or left as the examiner faces the person, i.e. in the coronal plane.[81]
Scoliosis has been described as a biomechanical deformity, the progression of which depends on asymmetric forces otherwise known as the Hueter-Volkmann Law.[29]
Management[edit]
Scoliosis curves do not straighten out on their own. Many children have slight curves that do not need treatment. In these cases, the children grow up to lead normal body posture by itself, even though their small curves never go away. If the patient has a larger curve and they are still growing, it is important to monitor the curve for change by periodic examination and standing x-rays as needed. The rise in spinal abnormalities require examination by an orthopaedic surgeon to determine if active treatment is needed.[82]
The traditional medical management of scoliosis is complex and is determined by the severity of the curvature and skeletal maturity, which together help predict the likelihood of progression.
The conventional options for children and adolescents are:[83]
- Observation
- Bracing
- Surgery
- Physical Therapy. Evidence suggests use of scoliosis specific exercises might prevent the progression of the curve along with possible bracing and surgery avoidance.[84]
For adults, treatment usually focuses on relieving any pain:[85][86]
- Pain medication
- Posture checking
- Bracing
- Surgery[87]
Treatment for idiopathic scoliosis also depends upon the severity of the curvature, the spine’s potential for further growth, and the risk that the curvature will progress. Mild scoliosis (less than 30° deviation) and moderate scoliosis (30–45°) can typically be treated conservatively with bracing in conjunction with scoliosis-specific exercises.[4] Severe curvatures that rapidly progress may require surgery with spinal rod placement and spinal fusion. In all cases, early intervention offers the best results.[citation needed]
A specific type of physical therapy may be useful.[88][4] Evidence to support their use however is weak.[2][12] Low quality evidence suggests scoliosis-specific exercises (SSE) may be more effective than electrostimulation.[89] Evidence for the Schroth method is insufficient to support its use.[90] Significant improvement in function, vertebral angles and trunk asymmetries have been recorded following the implementation of Schroth method in terms of conservative management of scoliosis. Some other forms of exercises interventions have been lately used in the clinical practice for therapeutic management of scoliosis such as global postural reeducation and the Klapp method.[84]
Bracing[edit]
A Chêneau brace achieving correction from 56° to 27° Cobb angle
Bracing is normally done when the person has bone growth remaining and is, in general, implemented to hold the curve and prevent it from progressing to the point where surgery is recommended. In some cases with juveniles, bracing has reduced curves significantly, going from a 40° (of the curve, mentioned in length above) out of the brace to 18°. Braces are sometimes prescribed for adults to relieve pain related to scoliosis. Bracing involves fitting the person with a device that covers the torso; in some cases, it extends to the neck (example being the Milwaukee Brace).[91]
Female adolescent (14 years old) patient wearing a Milwaukee brace — with neck ring and mandible (chin) pad showing
The most commonly used brace is a TLSO, such as a Boston brace, a corset-like an appliance that fits from armpits to hips and is custom-made from fiberglass or plastic. It is typically recommended to be worn 22–23 hours a day, and applies pressure on the curves in the spine. The effectiveness of the brace depends on not only brace design and orthotist skill, but also people’s compliance and amount of wear per day. An alternative form of brace is a nighttime only brace, that is worn only at night whilst the child sleeps, and which overcorrects the deformity.[92] Whilst nighttime braces are more convenient for children and families, it is unknown if the effectiveness of the brace is as good as conventional braces. The UK government have funded a large clinical trial (called the BASIS study) to resolve this uncertainty.[93] The BASIS study is ongoing throughout the UK in all of the leading UK children’s hospitals that treat scoliosis, with families encouraged to take part.
Indications for bracing: people who are still growing who present with Cobb angles less than 20° should be closely monitored. People who are still growing who present with Cobb angles of 20 to 29° should be braced according to the risk of progression by considering age, Cobb angle increase over a six-month period, Risser sign, and clinical presentation. People who are still growing who present with Cobb angles greater than 30° should be braced. However, these are guidelines and not every person will fit into this table.
For example, a person who is still growing with a 17° Cobb angle and significant thoracic rotation or flatback could be considered for nighttime bracing. On the opposite end of the growth spectrum, a 29° Cobb angle and a Risser sign three or four might not need to be braced because the potential for progression is reduced.[94] The Scoliosis Research Society’s recommendations for bracing include curves progressing to larger than 25°, curves presenting between 30 and 45°, Risser sign 0, 1, or 2 (an X-ray measurement of a pelvic growth area), and less than six months from the onset of menses in girls.[95]
Scoliosis braces are usually comfortable, especially when well designed and well fitted, also after the 7- to 10-day break-in period. A well fitted and functioning scoliosis brace provides comfort when it is supporting the deformity and redirecting the body into a more corrected and normal physiological position.[96]
Evidence supports that bracing prevents worsening of disease, but whether it changes quality of life, appearance, or back pain is unclear.[97]
Surgery[edit]
Preoperative (left) and postoperative (right) X-ray of a person with thoracic dextroscoliosis and lumbar levoscoliosis: The X-ray is usually projected anteroposterior, such that the right side of the subject is on the right side of the image; i.e., the subject is viewed from the rear (see left image; the right image is seen from the front). This projection is typically used by spine surgeons, as it is how surgeons see their patients when they are on the operating table (in the prone position). This is the opposite of many Chest radiographs, where the image is posteroanterior, i.e. projected as if looking at the patient from the front. The surgery was a fusion with instrumentation.[citation needed]
Surgery is usually recommended by orthopedists for curves with a high likelihood of progression (i.e., greater than 45 to 50° of magnitude), curves that would be cosmetically unacceptable as an adult, curves in people with spina bifida and cerebral palsy that interfere with sitting and care, and curves that affect physiological functions such as breathing.[98]
Surgery is indicated by the Society on Scoliosis Orthopaedic and Rehabilitation Treatment (SOSORT) at 45 to 50°[4] and by the Scoliosis Research Society (SRS) at a Cobb angle of 45°.[99] SOSORT uses the 45 to 50° threshold as a result of the well-documented, plus or minus 5° measurement error that can occur while measuring Cobb angles.[citation needed]
Surgeons who are specialized in spine surgery perform surgery for scoliosis. To completely straighten a scoliotic spine is usually impossible, but for the most part, significant corrections are achieved.[100]
The two main types of surgery are:[citation needed]
- Anterior fusion: This surgical approach is through an incision at the side of the chest wall.
- Posterior fusion: This surgical approach is through an incision on the back and involves the use of metal instrumentation to correct the curve.
One or both of these surgical procedures may be needed. The surgery may be done in one or two stages and, on average, takes four to eight hours.
A new tethering procedure (anterior vertebral body tethering) may be appropriate for some patients.
Prognosis[edit]
A 50-year follow-up study published in the Journal of the American Medical Association (2003) asserted the lifelong physical health, including cardiopulmonary and neurological functions, and mental health of people with idiopathic scoliosis are comparable to those of the general population. Scoliosis that interferes with normal systemic functions is «exceptional»[101] and «rare», and «untreated [scoliosis] people had similar death rates and were just as functional and likely to lead productive lives 50 years after diagnosis as people with normal spines.»[22][102] In an earlier University of Iowa follow-up study, 91% of people with idiopathic scoliosis displayed normal pulmonary function, and their life expectancy was found to be 2% more than that of the general population.[23] Later (2006-) studies corroborate these findings, adding that they are «reassuring for the adult patient who has adolescent onset idiopathic scoliosis in approximately the 50–70° range.»[103] These modern landmark studies supersede earlier studies (e.g. Mankin-Graham-Schauk 1964) that did implicate moderate idiopathic scoliosis in impaired pulmonary function.[citation needed]
Generally, the prognosis of scoliosis depends on the likelihood of progression. The general rules of progression are larger curves carry a higher risk of progression than smaller curves, and thoracic and double primary curves carry a higher risk of progression than single lumbar or thoracolumbar curves. In addition, people not having yet reached skeletal maturity have a higher likelihood of progression (i.e., if the person has not yet completed the adolescent growth spurt).[104]
Epidemiology[edit]
Scoliosis affects 2–3% of the United States population, which is equivalent to about five to nine million cases.[4] A scoliosis spinal column curve of 10° or less affects 1.5% to 3% of individuals.[95] The age of onset is usually between 10 years and 15 years (can occur at a younger age) in children and adolescents, making up to 85% of those diagnosed. This is seen to be due to rapid growth spurts occurring at puberty when spinal development is most relenting to genetic and environmental influences.[105] Because female adolescents undergo growth spurts before postural musculoskeletal maturity, scoliosis is more prevalent among females.[106]
Although fewer cases are present today using Cobb angle analysis for diagnosis, scoliosis remains a prevailing condition, appearing in otherwise healthy children. Despite the fact that scoliosis is a disfigurement of the spine, it has been shown to influence the pneumonic function, balance while standing and stride execution of kids with scoliosis. The impacts of backpack carriage on these three side effects have been broadly researched.[107] Incidence of idiopathic scoliosis (IS) stops after puberty when skeletal maturity is reached, however, further curvature may proceed during late adulthood due to vertebral osteoporosis and weakened musculature.[4]
History[edit]
Female with lateral curvature of the spine
Ever since the condition was discovered by the Greek physician Hippocrates, a cure has been sought. Treatments such as bracing and the insertion of rods into the spine were employed during the 1900s. In the mid-20th century, new treatments and improved screening methods have been developed to reduce the progression of scoliosis in patients and alleviate their associated pain. School children were during this period believed to develop poor posture as a result of working at their desks, and many were diagnosed with scoliosis. It was also considered to be caused by tuberculosis or poliomyelitis, diseases that were successfully managed using vaccines and antibiotics.[citation needed]
The American orthopaedic surgeon Alfred Shands Jr. discovered that two percent of patients had non-disease related scoliosis, later termed idiopathic scoliosis, or the «cancer of orthopaedic surgery». These patients were treated with questionable remedies.[108] A theory at the time—now discredited—was that the condition needed to be detected early to halt its progression, and so some schools made screening for scoliosis mandatory. Measurements of shoulder height, leg length and spinal curvature were made, and the ability to bend forwards, along with body posture, was tested, but students were sometimes misdiagnosed because of their poor posture.[citation needed]
An early treatment was the Milwaukee brace, a rigid contraption of metal rods attached to a plastic or leather girdle, designed to straighten the spine. Because of the constant pressure applied to the spine, the brace was uncomfortable. It caused jaw and muscle pain, skin irritation, as well as low self-esteem.[citation needed]
Surgery[edit]
In 1962, the American orthopaedic surgeon Paul Harrington introduced a metal spinal system of instrumentation that assisted with straightening the spine, as well as holding it rigid while fusion took place. The now obsolete Harrington rod operated on a ratchet system, attached by hooks to the spine at the top and bottom of the curvature that when cranked would distract—or straighten—the curve. The Harrington rod obviates the need for prolonged casting, allowing patients greater mobility in the postoperative period and significantly reducing the quality of life burden of fusion surgery. The Harrington rod was the precursor to most modern spinal instrumentation systems. A major shortcoming was that it failed to produce a posture wherein the skull would be in proper alignment with the pelvis, and it did not address rotational deformity. As the person aged, there would be increased wear and tear, early onset arthritis, disc degeneration, muscular stiffness, and acute pain. «Flatback» became the medical name for a related complication, especially for those who had lumbar scoliosis.[109]
In the 1960s, the gold standard for idiopathic scoliosis was a posterior approach using a single Harrington rod. Post-operative recovery involved bed rest, casts, and braces. Poor results became apparent over time.[110]
In the 1970s, an improved technique was developed using two rods and wires attached at each level of the spine. This segmented instrumentation system allowed patients to become mobile soon after surgery.[110]
In the 1980s, Cotrel-Dubousset instrumentation improved fixation and addressed sagittal imbalance and rotational defects unresolved by the Harrington rod system. This technique used multiple hooks with rods to give stronger fixation in three dimensions, usually eliminating the need for postoperative bracing.[110]
Evolution[edit]
A 14–15th-century woman who had severe scoliosis, and died at about 35 years, Limburgs Museum Venlo
There are links between human spinal morphology, bipedality, and scoliosis which suggest an evolutionary basis for the condition. Scoliosis has not been found in chimpanzees or gorillas.[111] Thus, it has been hypothesized that scoliosis may actually be related to humans’ morphological differences from these apes.[111] Other apes have a shorter and less mobile lower spine than humans. Some of the lumbar vertebrae in Pan are «captured», meaning that they are held fast between the ilium bones of the pelvis. Compared to humans, Old World monkeys have far larger erector spinae muscles, which are the muscles which hold the spine steady.[111] These factors make the lumbar spine of most primates less flexible and far less likely to deviate than those of humans. While this may explicitly relate only to lumbar scolioses, small imbalances in the lumbar spine could precipitate thoracic problems as well.[111]
Scoliosis may be a byproduct of strong selection for bipedalism. For a bipedal stance, a highly mobile, elongated lower spine is very beneficial.[111] For instance, the human spine takes on an S-shaped curve with lumbar lordosis, which allows for better balance and support of an upright trunk.[112] Selection for bipedality was likely strong enough to justify the maintenance of such a disorder. Bipedality is hypothesized to have emerged for a variety of different reasons, many of which would have certainly conferred fitness advantages. It may increase viewing distance, which can be beneficial in hunting and foraging as well as protection from predators or other humans; it makes long-distance travel more efficient for foraging or hunting; and it facilitates terrestrial feeding from grasses, trees, and bushes.[113] Given the many benefits of bipedality which depends on a particularly formed spine, it is likely that selection for bipedalism played a large role in the development of the spine as we see it today, in spite of the potential for «scoliotic deviations».[111] According to the fossil record, scoliosis may have been more prevalent among earlier hominids such as Australopithecus and Homo erectus, when bipedality was first emerging. Their fossils indicate that there may have been selected over time for a slight reduction in lumbar length to what we see today, favouring a spine that could efficiently support bipedality with a lower risk of scoliosis.[111]
Society and culture[edit]
The cost of scoliosis involves both monetary losses and lifestyle limitations that increase with severity. Respiratory deficiencies may also arise from thoracic deformities and cause abnormal breathing.[114] This directly affects exercise and work capacity, decreasing the overall quality of life.[4]
In the health care system of the United States, the average hospital cost for cases involving surgical procedures was $30,000 to $60,000 per person in 2010.[115] As of 2006, the cost of bracing has been published as up to $5,000 during rapid growth periods, when braces must be consistently replaced across multiple follow-ups.[4]
Research[edit]
Genetic testing for adolescent idiopathic scoliosis, which became available in 2009 and is still under investigation, attempts to gauge the likelihood of curve progression.[116][needs update]
See also[edit]
- Back brace
- Kyphosis
- Lordosis
- Neuromechanics of idiopathic scoliosis
- Pott disease
- Scheuermann’s disease
- Schooliosis
- Scoliosis Research Society
References[edit]
- ^ «Scoliosis». Merriam Webster. Archived from the original on 11 August 2016. Retrieved 12 August 2016.
- ^ a b c d e f g h i j k l m n o p q r s t «Questions and Answers about Scoliosis in Children and Adolescents». NIAMS. December 2015. Archived from the original on 25 August 2016. Retrieved 12 August 2016.
- ^ a b c d e f «Adolescent idiopathic scoliosis». Genetics Home Reference. September 2013. Archived from the original on 16 August 2016. Retrieved 12 August 2016.
- ^ a b c d e f g h i j Negrini S, Donzelli S, Aulisa AG, Czaprowski D, Schreiber S, de Mauroy JC, et al. (2018). «2016 SOSORT guidelines: orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth». Scoliosis and Spinal Disorders. 13: 3. doi:10.1186/s13013-017-0145-8. PMC 5795289. PMID 29435499.
- ^ a b Shakil H, Iqbal ZA, Al-Ghadir AH (2014). «Scoliosis: review of types of curves, etiological theories and conservative treatment». Journal of Back and Musculoskeletal Rehabilitation. 27 (2): 111–115. doi:10.3233/bmr-130438. PMID 24284269.
- ^ «Scoliosis — Symptoms, Diagnosis and Treatment». aans.org. Retrieved 10 February 2022.
- ^ a b Illés TS, Lavaste F, Dubousset JF (April 2019). «The third dimension of scoliosis: The forgotten axial plane». Orthopaedics & Traumatology, Surgery & Research. 105 (2): 351–359. doi:10.1016/j.otsr.2018.10.021. PMID 30665877.
- ^ Yang S, Andras LM, Redding GJ, Skaggs DL (January 2016). «Early-Onset Scoliosis: A Review of History, Current Treatment, and Future Directions». Pediatrics. 137 (1): e20150709. doi:10.1542/peds.2015-0709. PMID 26644484. S2CID 557560.
- ^ Agabegi SS, Kazemi N, Sturm PF, Mehlman CT (December 2015). «Natural History of Adolescent Idiopathic Scoliosis in Skeletally Mature Patients: A Critical Review». The Journal of the American Academy of Orthopaedic Surgeons. 23 (12): 714–723. doi:10.5435/jaaos-d-14-00037. PMID 26510624. S2CID 6735774.
- ^ Berdishevsky H, Lebel VA, Bettany-Saltikov J, Rigo M, Lebel A, Hennes A, et al. (2016). «Physiotherapy scoliosis-specific exercises — a comprehensive review of seven major schools». Scoliosis and Spinal Disorders. 11: 20. doi:10.1186/s13013-016-0076-9. PMC 4973373. PMID 27525315.
- ^ Park JH, Jeon HS, Park HW (June 2018). «Effects of the Schroth exercise on idiopathic scoliosis: a meta-analysis». European Journal of Physical and Rehabilitation Medicine. 54 (3): 440–449. doi:10.23736/S1973-9087.17.04461-6. PMID 28976171. S2CID 39497372.
- ^ a b Thompson JY, Williamson EM, Williams MA, Heine PJ, Lamb SE (June 2019). «Effectiveness of scoliosis-specific exercises for adolescent idiopathic scoliosis compared with other non-surgical interventions: a systematic review and meta-analysis». Physiotherapy. 105 (2): 214–234. doi:10.1016/j.physio.2018.10.004. PMID 30824243. S2CID 73471547.
- ^ «scoliosis». Dictionary.com Unabridged (Online). n.d. Retrieved 12 August 2016. Archived 16 August 2016 at the Wayback Machine.
- ^ Aebi, Max (2005). «The Adult Scoliosis» (PDF). European Spine Journal. 14 (10): 925–948. doi:10.1007/s00586-005-1053-9. PMID 16328223. S2CID 22119278. Retrieved 21 December 2022.
- ^ a b Nachemson, Alf (1968). «A Long Term Follow-up Study of Non-treated Scoliosis». Acta Orthopaedica Scandinavica. 39 (4): 466–476. doi:10.3109/17453676808989664. PMID 5726117. Retrieved 21 December 2022.
- ^ Yanner, Baher S. (17 December 2021). «How Scoliosis Affects the Body». spineina.com. Spine Institute of North America. Retrieved 8 January 2023.
- ^ «Muscular Imbalance: Why Does Scoliosis Create One Weak Side?». www.scoliosissos.com. Scoliosis SOS Clinic. 28 August 2017. Retrieved 10 January 2023.
- ^ a b Coillard, Christine; Leroux, Michel A.; Prince, François; Rivard, Charles H.; Zabjek, Karl Franc (2008). «Postural Characteristics of Adolescents With Idiopathic Scoliosis». Journal of Pediatric Orthopaedics. 28 (2): 218–224. doi:10.1097/BPO.0b013e3181651bdc. PMID 18388718. S2CID 34046217. Retrieved 8 January 2023.
- ^ Giachelli CM (March 1999). «Ectopic calcification: gathering hard facts about soft tissue mineralization». The American Journal of Pathology. 154 (3): 671–675. doi:10.1016/S0002-9440(10)65313-8. PMC 1866412. PMID 10079244.
- ^ Thometz JG, Simon SR (October 1988). «Progression of scoliosis after skeletal maturity in institutionalized adults who have cerebral palsy». The Journal of Bone and Joint Surgery. American Volume. 70 (9): 1290–1296. doi:10.2106/00004623-198870090-00002. PMID 3182881.
- ^ Koumbourlis AC (June 2006). «Scoliosis and the respiratory system». Paediatric Respiratory Reviews. 7 (2): 152–160. doi:10.1016/j.prrv.2006.04.009. PMID 16765303.
- ^ a b Weinstein SL, Dolan LA, Spratt KF, Peterson KK, Spoonamore MJ, Ponseti IV (February 2003). «Health and function of patients with untreated idiopathic scoliosis: a 50-year natural history study». JAMA. 289 (5): 559–567. doi:10.1001/jama.289.5.559. PMID 12578488.
- ^ a b Weinstein SL, Zavala DC, Ponseti IV (June 1981). «Idiopathic scoliosis: long-term follow-up and prognosis in untreated patients». The Journal of Bone and Joint Surgery. American Volume. 63 (5): 702–712. doi:10.2106/00004623-198163050-00003. PMID 6453874. S2CID 22429772.
- ^ Trobisch P, Suess O, Schwab F (December 2010). «Idiopathic scoliosis». Deutsches Ärzteblatt International. 107 (49): 875–83, quiz 884. doi:10.3238/arztebl.2010.0875. PMC 3011182. PMID 21191550.
It was once assumed, on the basis of studies in heterogeneous patient populations, that patients with untreated adolescent scoliosis would necessarily become wheelchair-dependent in old age and were likely to die of cardiopulmonary arrest for reasons related to scoliosis. This is no longer held to be the case.
- ^ Agabegi ED, Agabegi SS (2008). Step-Up to Medicine. Step-Up Series. Hagerstwon, MD: Lippincott Williams & Wilkins. p. 90. ISBN 978-0-7817-7153-5.
- ^ a b c d Gorman KF, Julien C, Moreau A (October 2012). «The genetic epidemiology of idiopathic scoliosis». European Spine Journal. 21 (10): 1905–1919. doi:10.1007/s00586-012-2389-6. PMC 3463687. PMID 22695700.
- ^ a b Ogilvie JW, Braun J, Argyle V, Nelson L, Meade M, Ward K (March 2006). «The search for idiopathic scoliosis genes». Spine. 31 (6): 679–681. doi:10.1097/01.brs.0000202527.25356.90. PMID 16540873. S2CID 24280322.
- ^ Montanaro L, Parisini P, Greggi T, Di Silvestre M, Campoccia D, Rizzi S, Arciola CR (December 2006). «Evidence of a linkage between matrilin-1 gene (MATN1) and idiopathic scoliosis». Scoliosis. 1: 21. doi:10.1186/1748-7161-1-21. PMC 1769398. PMID 17176459.
- ^ a b Ogilvie J (February 2010). «Adolescent idiopathic scoliosis and genetic testing». Current Opinion in Pediatrics. 22 (1): 67–70. doi:10.1097/MOP.0b013e32833419ac. PMID 19949338. S2CID 1044562.
- ^ Cheng JC, Castelein RM, Chu WC, Danielsson AJ, Dobbs MB, Grivas TB, et al. (September 2015). «Adolescent idiopathic scoliosis». Nature Reviews. Disease Primers. 1: 15030. doi:10.1038/nrdp.2015.30. PMID 27188385. S2CID 21284193.
- ^ Burwell RG (2003). «Aetiology of idiopathic scoliosis: current concepts». Pediatric Rehabilitation. 6 (3–4): 137–170. doi:10.1080/13638490310001642757. PMID 14713582. S2CID 12154979.
- ^ Shahidi B, Yoo A, Farnsworth C, Newton PO, Ward SR (September 2021). «Paraspinal muscle morphology and composition in adolescent idiopathic scoliosis: A histological analysis». JOR Spine. 4 (3): e1169. doi:10.1002/jsp2.1169. PMC 8479518. PMID 34611591.
- ^ Kouwenhoven JW, Castelein RM (December 2008). «The pathogenesis of adolescent idiopathic scoliosis: review of the literature». Spine. 33 (26): 2898–2908. doi:10.1097/BRS.0b013e3181891751. PMID 19092622. S2CID 19749217.
- ^ Weiss HR, Goodall D (August 2008). «Rate of complications in scoliosis surgery — a systematic review of the Pub Med literature». Scoliosis. 3: 9. doi:10.1186/1748-7161-3-9. PMC 2525632. PMID 18681956.
- ^ Fischer CR, Kim Y (July 2011). «Selective fusion for adolescent idiopathic scoliosis: a review of current operative strategy». European Spine Journal. 20 (7): 1048–1057. doi:10.1007/s00586-011-1730-9. PMC 3176697. PMID 21387194.
- ^ Merola AA, Haher TR, Brkaric M, Panagopoulos G, Mathur S, Kohani O, et al. (September 2002). «A multicenter study of the outcomes of the surgical treatment of adolescent idiopathic scoliosis using the Scoliosis Research Society (SRS) outcome instrument». Spine. 27 (18): 2046–2051. doi:10.1097/00007632-200209150-00015. PMID 12634567.
- ^ Chen Z, Rong L (February 2016). «Comparison of combined anterior-posterior approach versus posterior-only approach in treating adolescent idiopathic scoliosis: a meta-analysis». European Spine Journal. 25 (2): 363–371. doi:10.1007/s00586-015-3968-0. PMID 25900299. S2CID 4434949.
- ^ a b Rapp van Roden EA, Richardson RT, Russo SA, Rose WC, Nicholson KF, Chafetz RS, et al. (January 2019). «Analysis of Shoulder Complex Function After Posterior Spinal Fusion in Adolescents With Idiopathic Scoliosis». Journal of Pediatric Orthopedics. 39 (1): e32–e38. doi:10.1097/BPO.0000000000001267. PMID 30312252. S2CID 52975845.
- ^ Bastrom TP, Marks MC, Yaszay B, Newton PO, et al. (Harms Study Group) (October 2013). «Prevalence of postoperative pain in adolescent idiopathic scoliosis and the association with preoperative pain». Spine. 38 (21): 1848–1852. doi:10.1097/brs.0b013e3182a4aa97. PMID 23883827.
- ^ Landman Z, Oswald T, Sanders J, Diab M, et al. (Spinal Deformity Study Group) (May 2011). «Prevalence and predictors of pain in surgical treatment of adolescent idiopathic scoliosis». Spine. 36 (10): 825–829. doi:10.1097/brs.0b013e3181de8c2b. PMID 21192302. S2CID 205514923.
- ^ Rubery PT, Bradford DS (February 2002). «Athletic activity after spine surgery in children and adolescents: results of a survey». Spine. 27 (4): 423–427. doi:10.1097/00007632-200202150-00019. PMID 11840110. S2CID 19524978.
- ^ Tarrant RC, O’Loughlin PF, Lynch S, Queally JM, Sheeran P, Moore DP, Kiely PJ (August 2014). «Timing and predictors of return to short-term functional activity in adolescent idiopathic scoliosis after posterior spinal fusion: a prospective study». Spine. 39 (18): 1471–1478. doi:10.1097/brs.0000000000000452. PMID 24875955. S2CID 35816768.
- ^ a b c Trobisch P, Suess O, Schwab F (December 2010). «Idiopathic scoliosis». Deutsches Ärzteblatt International. 107 (49): 875–83, quiz 884. doi:10.3238/arztebl.2010.0875. PMC 3011182. PMID 21191550.
- ^ «What is Scoliosis: What Causes Scoliosis?». MedicalBug. 17 February 2012. Archived from the original on 9 April 2012. Retrieved 18 March 2012.
- ^ Scoliosis Research Society. (2014). Congenital Scoliosis. Scoliosis Research Society. «Congenital Scoliosis — Scoliosis Research Society (SRS)». Archived from the original on 1 July 2014. Retrieved 21 May 2014.
- ^ Trontelj JV, Pecak F, Dimitrijević MR (August 1979). «Segmental neurophysiological mechanisms in scoliosis». The Journal of Bone and Joint Surgery. British Volume. 61-B (3): 310–313. doi:10.1302/0301-620x.61b3.479254. PMID 479254.
- ^ POSNA. (2014). Neuromuscular Scoliosis. The Pediatric Orthopaedic Society of North America. «Neuromuscular Scoliosis — POSNA». Archived from the original on 21 May 2014. Retrieved 21 May 2014.
- ^ Chung AS, Renfree S, Lockwood DB, Karlen J, Belthur M (November 2019). «Syndromic Scoliosis: National Trends in Surgical Management and Inpatient Hospital Outcomes: A 12-Year Analysis». Spine. 44 (22): 1564–1570. doi:10.1097/BRS.0000000000003134. PMID 31689252. S2CID 201175687.
- ^ Komazec, Jovan; Matic, Aleksandra (2009). «Amniotic Band Syndrome» (PDF). Acta Medica Medianae. 48 (2): 44–48. Retrieved 29 January 2023.
- ^ «Chiari malformation». mayoclinic.org. Mayo Clinic. Retrieved 29 January 2023.
- ^ Marchesi, Chiara; Pareyson, Davide (2009). «Diagnosis, natural history, and management of Charcot-Marie-Tooth disease» (PDF). The Lancet Neurology. 8 (7): 654–667. doi:10.1016/S1474-4422(09)70110-3. PMID 19539237. S2CID 665324. Retrieved 29 January 2023.
- ^ Krigger, Karen W. (2006). «Celebral Palsy: An Overview». American Family Physician. 73 (1): 91–100. PMID 16417071. Retrieved 29 January 2023.
- ^ Chandraekharan, Praveen Kumar; Lakshminrusimha, Satyan; Madappa, Rajeshwari; Rawat, Munmun; Rothstein, David H. (2017). «Congenital Diaphragmatic hernia — a review». Maternal Health, Neonatology and Perinatology. 3: 6. doi:10.1186/s40748-017-0045-1. PMC 5356475. PMID 28331629.
- ^ a b c Hresko, M. Timothy (2013). «Idiopathic Scoliosis in Adolescents» (PDF). The New England Journal of Medicine. 368 (9): 834–841. doi:10.1056/NEJMcp1209063. PMID 23445094. Retrieved 29 January 2023.
- ^ Aartsma-Ra, Annemieke; Duan, Dongsheng; Goemans, Nathalie; Mercuri, Eugenio; Takeda, Shin’ichi (2021). «Duchenne muscular dystrophy». Nature Reviews Disease Primers. 7.
- ^ Fuente-Mora, Cristina; Kauffman, Horacio; Mendoza-Santiesteban, Carlos; Norcliffe-Kauffman, Lucy; Palma, Jose-Alberto; Percival, Leila (2014). «Current treatments in familial dysautonomia». Expert Opinion on Pharmacotherapy. 15 (18): 2653–2671. doi:10.1517/14656566.2014.970530. PMC 4236240. PMID 25323828. Retrieved 29 January 2023.
- ^ Blake, Kim D; Prasad, Chitra (2006). «CHARGE syndrome». Orphanet Journal of Rare Diseases. 1: 34. doi:10.1186/1750-1172-1-34. PMC 1586184. PMID 16959034.
- ^ «Fragile X syndrome». Department for Work and Pensions, UK. Archived from the original on 19 March 2012. Retrieved 29 August 2011.
- ^ Davids JR, Hagerman RJ, Eilert RE (July 1990). «Orthopaedic aspects of fragile-X syndrome». The Journal of Bone and Joint Surgery. American Volume. 72 (6): 889–896. doi:10.2106/00004623-199072060-00015. PMID 2195034.
- ^ Delatycki, Martin B; Forrest, Susan M; Williamson, Robert (2000). «Freidreich ataxia: an overview» (PDF). Journal of Medical Genetics. 37 (1): 1–8. doi:10.1136/jmg.37.1.1. PMC 1734457. PMID 10633128. Retrieved 30 January 2023.
- ^ Sheth, Ujash (2021). «Hemihypertrophy». www.orthobullets.com. OrthoBullets. Retrieved 31 January 2023.
- ^ Black, James H.; Bowdin, Sarah; Dietz, Harry C.; El-Hamamsy, Ismail; Frischmeyer-Guerrerio, Pamela A.; Guerrerio, Anthony L.; Loeys, Bart; MacCarrick, Gretchen; Sponseller, Paul D (2014). «Loeys-Dietz syndrome: a primer for diagnosis and management». Genetics in Medicine. 16 (8): 576–587. doi:10.1038/gim.2014.11. PMC 4131122. PMID 24577266.
- ^ Fryer, G; Green, A; McIntosh, I; Mountford, R; Sweeney, E (2003). «Nail patella syndrome: a review of the phenotype aided by developmental biology» (PDF). Journal of Medical Genetics. 40 (3): 153–162. doi:10.1136/jmg.40.3.153. PMC 1735400. PMID 12624132. Retrieved 30 January 2023.
- ^ Boyd, Kevin P.; Korf, Bruce R.; Theos, Amy (2009). «Neurofibromatosis type 1». Journal of the American Academy of Dermatology. 61 (1): 1–16. doi:10.1016/j.jaad.2008.12.051. PMC 2716546. PMID 19539839.
- ^ Glorieux, Francis H; Rauch, Frank (2004). «Osteogenesis imperfecta» (PDF). The Lancet. 363 (9418): 1377–1385. doi:10.1016/S0140-6736(04)16051-0. PMID 15110498. S2CID 24081895. Retrieved 30 January 2023.
- ^ Cassidy, Suzanne B.; Driscoll, Daniel J.; Miller, Jennifer L.; Schwartz, Stuart (2012). «Prader-Willi syndrome». Genetics in Medicine. 14 (1): 10–26. doi:10.1038/gim.0b013e31822bead0. PMID 22237428. S2CID 19992. Retrieved 30 January 2023.
- ^ Biesecker, Leslie G.; Choyke, Peter L.; Jamis-Dow, Carlos A.; Turner, Joyce (2004). «Radiologic Manifestations of Proteus Syndrome» (PDF). RadioGraphics. 24 (4): 1051–1068. doi:10.1148/rg.244035726. PMID 15256628. Retrieved 31 January 2023.
- ^ Adzick, N Scott; Melchionne, Jeanne; Mitchell, Laura E; Pasquariello, Patrick S; Sutton, Leslie N; Whitehead, Alexander S (2004). «Spina bifida». The Lancet. 364 (9448): 1885–1895. doi:10.1016/S0140-6736(04)17445-X. PMID 15555669. S2CID 37770338. Retrieved 31 January 2023.
- ^ Lunn, Mitchell R; Wang, Ching H (2008). «Spinal muscular atrophy». The Lancet. 371 (9630): 2120–2133. doi:10.1016/S0140-6736(08)60921-6. PMID 18572081. S2CID 11023418. Retrieved 31 January 2023.
- ^ Vandertop, W. Peter (2014). «Syringomyelia». Neuropediatrics. 45 (1): 003–009. doi:10.1055/s-0033-1361921. PMID 24272770. Retrieved 31 January 2023.
- ^ Desmarais, Thomas J.; Keller, Martin S. (2013). «Pectus carinatum» (PDF). Current Opinion in Pediatrics. 25 (3): 375–381. doi:10.1097/MOP.0b013e3283604088. PMID 23657247. S2CID 46604820. Retrieved 31 January 2023.
- ^ Giradi, Federico; Hughes, Alex; Kotwal, Suhel; Pumberger, Matthias (2011). «Degenerative Scoliosis: A Review». HSS Journal. 7 (3): 257–264. doi:10.1007/s11420-011-9204-5. PMC 3192887. PMID 23024623.
- ^ «Scoliosis symptoms – pain, flat back, screening, self-assessment». iscoliosis.com.
- ^ «Scoliometer (Inclinometer)». National Scoliosis Foundation. Archived from the original on 21 November 2014.
- ^ Kim H, Kim HS, Moon ES, Yoon CS, Chung TS, Song HT, et al. (November 2010). «Scoliosis imaging: what radiologists should know». Radiographics. 30 (7): 1823–1842. doi:10.1148/rg.307105061. PMID 21057122.
The main purpose of performing CT or MR imaging in a patient with scoliosis is to identify an underlying cause. MR imaging is used with increasing frequency to evaluate patients with an unusual curve pattern or alarming clinical manifestations. Nevertheless, two reasons for performing such screening are plausible: First, the treatment of an underlying neurologic lesion could help alleviate progressive neurologic deterioration and lead to improvement or stabilization of scoliosis; second, surgery performed to correct scoliosis in the presence of an underlying neurologic disorder that has not been identified and treated could result in new or additional neurologic deficits.
- ^ Oakley PA, Ehsani NN, Harrison DE (1 April 2019). «The Scoliosis Quandary: Are Radiation Exposures From Repeated X-Rays Harmful?». Dose-Response. 17 (2): 1559325819852810. doi:10.1177/1559325819852810. PMC 6560808. PMID 31217755.
- ^ «Early Onset Scoliosis | Scoliosis Research Society». www.srs.org. Archived from the original on 21 June 2016. Retrieved 10 July 2016.
- ^ Sponseller PD, Yazici M, Demetracopoulos C, et al. Evidence basisfor management of spine and chest wall deformities in children.Spine(Phila Pa 1976). 2007;32(suppl):S81–S90
- ^ Celebioglu E., Yataganbaba A., Bekmez S., et al Growing-rod Graduates with Idiopathic Early-onset Scoliosis Have Comparable Exercise Tolerance to Patients with Surgically Treated Adolescent Idiopathic Scoliosis. J. Pediatr. Orthop.. 2020;40(8):e734-e739. doi:10.1097/BPO.0000000000001567
- ^ Grossman DC, Curry SJ, Owens DK, Barry MJ, Davidson KW, Doubeni CA, et al. (January 2018). «Screening for Adolescent Idiopathic Scoliosis: US Preventive Services Task Force Recommendation Statement». JAMA. 319 (2): 165–172. doi:10.1001/jama.2017.19342. PMID 29318284. S2CID 38852032.
- ^ Lau K. The Complete Scoliosis Surgery Handbook for Patients: An In-Depth and Unbiased Look Into What to Expect Before and During Scoliosis Surgery. Health In Your Hands. p. 89. ISBN 978-9810785925.
- ^ «Treatment Options | Scoliosis Research Society». www.srs.org. Retrieved 11 February 2022.
- ^ «Treating scoliosis in children». NHS Choices. 19 February 2013. Archived from the original on 14 May 2014. Retrieved 14 May 2014.
- ^ a b Ceballos Laita L, Tejedor Cubillo C, Mingo Gómez T, Jiménez Del Barrio S (August 2018). «Effects of corrective, therapeutic exercise techniques on adolescent idiopathic scoliosis. A systematic review». Archivos Argentinos de Pediatria. 116 (4): e582–e589. doi:10.5546/aap.2018.eng.e582. PMID 30016036.
- ^ «Scoliosis – Treatment in adults». NHS Choices. 19 February 2013. Archived from the original on 14 May 2014. Retrieved 14 May 2014.
- ^ «Idiopathic Scoliosis – Adult Nonoperative Management». Scoliosis Research Society. Archived from the original on 1 July 2014. Retrieved 14 May 2014.
- ^ «Idiopathic Scoliosis – Adult Surgical Treatment». Scoliosis Research Society. Archived from the original on 1 July 2014. Retrieved 14 May 2014.
- ^ Negrini S, Fusco C, Minozzi S, Atanasio S, Zaina F, Romano M (2008). «Exercises reduce the progression rate of adolescent idiopathic scoliosis: results of a comprehensive systematic review of the literature». Disability and Rehabilitation. 30 (10): 772–785. doi:10.1080/09638280801889568. PMID 18432435. S2CID 13188152.
- ^ Romano M, Minozzi S, Bettany-Saltikov J, Zaina F, Chockalingam N, Kotwicki T, et al. (August 2012). «Exercises for adolescent idiopathic scoliosis». The Cochrane Database of Systematic Reviews. 2012 (8): CD007837. doi:10.1002/14651858.cd007837.pub2. PMC 7386883. PMID 22895967.
- ^ Day JM, Fletcher J, Coghlan M, Ravine T (2019). «Review of scoliosis-specific exercise methods used to correct adolescent idiopathic scoliosis». Archives of Physiotherapy. 9: 8. doi:10.1186/s40945-019-0060-9. PMC 6708126. PMID 31463082.
- ^ The influence of elastic orthotic belt on sagittal profile in adolescent idiopathic thoracic scoliosis: A comparative radiographic study with Milwaukee brace., Research Gate, September 2010
- ^ Antoine L, Nathan D, Laure M, Briac C, Jean-François M, Corinne B (March 2020). «Compliance with night-time overcorrection bracing in adolescent idiopathic scoliosis: Result from a cohort follow-up». Medical Engineering & Physics. 77: 137–141. doi:10.1016/j.medengphy.2020.01.003. PMID 31992499. S2CID 210945485.
- ^ «BASIS study».
- ^ Wood G (2013). «To Brace or Not to Brace: The Three-Dimensional Nature and Growth Considerations for Adolescent Idiopathic Scoliosis». Academy Today (The Edge). American Academy of Orthosits and Prosthetist. pp. 5–8.
- ^ a b Herring JA (2002). Tachdjian’s Pediatric Orthopaedics. Philadelphia, PA: W.B. Saunders. ISBN 978-0-7216-5684-7.[page needed]
- ^ Wood GI (2013). The Cheneau Brace using Rigo Principles and the Wood Cheneau Rigo (WCR) Brace. Society on Scoliosis Orthopaedic and Rehabilitation Treatment (SOSORT). Chicago, IL.
- ^ Negrini S, Minozzi S, Bettany-Saltikov J, Chockalingam N, Grivas TB, Kotwicki T, et al. (June 2015). «Braces for idiopathic scoliosis in adolescents». The Cochrane Database of Systematic Reviews (6): CD006850. doi:10.1002/14651858.CD006850.pub3. hdl:2434/721317. PMID 26086959.
- ^ Alli RA (19 December 2020). «Scoliosis Treatment». WebMD. Retrieved 11 February 2020.
- ^ «Adolescent Idiopathic Scoliosis — Scoliosis Research Society (SRS)». Archived from the original on 16 January 2014. Retrieved 2 January 2014. adolescents/surgical_treatment.htm. Accessed 27 January 2013
- ^ Gibson I, Jagdish BN, Zhan G, Hajizedah K, Tho HK, Mengjie H, Dissanayake C (January 2012). «Development of a human spine simulation system.». In Yu W, Chattopadhyay S, Lim TC, Acharya UR (eds.). Advances in Therapeutic Engineering. CRC Press. p. 27. ISBN 978-1-4398-7174-4.
- ^ Hawes MC (May 2003). «Health and Function of Patients With Untreated Idiopathic Scoliosis—Reply». JAMA. 289 (20): 2644, author reply 2644–5. doi:10.1001/jama.289.20.2644-a. PMID 12771105.
- ^ «Many With Scoliosis Can Skip Treatments». stopgettingsick.com. Archived from the original on 20 August 2008.
- ^ Asher MA, Burton DC (March 2006). «Adolescent idiopathic scoliosis: natural history and long term treatment effects». Scoliosis. 1 (1): 2. doi:10.1186/1748-7161-1-2. PMC 1475645. PMID 16759428. S2CID 14194273.
- ^ «Adolescent Idiopathic Scoliosis | Scoliosis Research Society». www.srs.org. Retrieved 28 February 2018.
- ^ Edery P, Margaritte-Jeannin P, Biot B, Labalme A, Bernard JC, Chastang J, et al. (August 2011). «New disease gene location and high genetic heterogeneity in idiopathic scoliosis». European Journal of Human Genetics. 19 (8): 865–869. doi:10.1038/ejhg.2011.31. PMC 3172921. PMID 21407261.
- ^ Burwell RG (2003). «Aetiology of idiopathic scoliosis: current concepts». Pediatric Rehabilitation. 6 (3–4): 137–70. doi:10.1080/13638490310001642757. PMID 14713582. S2CID 12154979.
- ^ Bessette A, Rousseau CM, eds. (October 2012). Scoliosis : Causes, Symptoms and Treatment. Nova Science Publishers. ISBN 978-1-62081-007-1.
- ^ Linker B (April 2012). «A dangerous curve: the role of history in America’s scoliosis screening programs». American Journal of Public Health. 102 (4): 606–616. doi:10.2105/AJPH.2011.300531. PMC 3489358. PMID 22397340.
- ^ «Scoliosis Surgery». News-medical.net. 22 November 2009. Retrieved 16 January 2011.
- ^ a b c Bridwell K (8 February 2013). «Idiopathic Scoliosis: Options of Fixation and Fusion of Thoracic Curves». SpineUniverse. Retrieved 21 May 2014.
- ^ a b c d e f g Lovejoy CO (January 2005). «The natural history of human gait and posture. Part 1. Spine and pelvis». Gait & Posture. 21 (1): 95–112. doi:10.1016/s0966-6362(04)00014-1. PMID 15536039.
- ^ Harcourt-Smith WE (2007). «Chapter 5». Handbook of Paleoanthropology. Springer Berlin Heidelberg. pp. 1483–1518.
- ^ Hunt KD (March 1994). «The evolution of human bipedality: ecology and functional morphology». Journal of Human Evolution. 26 (3): 182–202. doi:10.1006/jhev.1994.1011.
- ^ Larson N (August 2011). «Early onset scoliosis: what the primary care provider needs to know and implications for practice». Journal of the American Academy of Nurse Practitioners. 23 (8): 392–403. doi:10.1111/j.1745-7599.2011.00634.x. PMID 21790832. S2CID 25902637.
- ^ Kamerlink JR, Quirno M, Auerbach JD, Milby AH, Windsor L, Dean L, et al. (May 2010). «Hospital cost analysis of adolescent idiopathic scoliosis correction surgery in 125 consecutive cases». The Journal of Bone and Joint Surgery. American Volume. 92 (5): 1097–1104. doi:10.2106/JBJS.I.00879. PMID 20439654.
- ^ Stenning M, Nelson I (2011). «Recent advances in the treatment of scoliosis in children». British Editorial Society of Bone and Joint Surgery. Archived from the original on 2 January 2014. Retrieved 1 January 2014.
External links[edit]
![]()
Wikimedia Commons has media related to Scoliosis.
- Scoliosis at Curlie
- Early Onset Scoliosis is the abnormal, side-to-side curve of the spine in children under five years old, often including children with congenital scoliosis (present at birth, with spine abnormalities) and infantile scoliosis (birth to three years).
- Questions and Answers about Scoliosis in Children and Adolescents – US National Institute of Arthritis and Musculoskeletal and Skin Diseases
Сколиоз
причины, симптомы, методы лечения и профилактики
Сколиоз — это трехплоскостная деформация позвоночника с нарушениями осанки . Позвоники поворачиваются вдоль вертикальной оси, происходит боковое искривление позвоночника. Заболевание развивается у детей, с возрастом прогрессирует и переходит в более тяжёлую форму. Также искривление возникает из-за неправильного развития плода в утробе матери, после серьёзных травм позвоночника или по другим причинам. Для лечения сколиоза нужно обращаться к ортопеду.

Разновидности
По этиологии:
- врождённая. Образуется из-за аномалий развития или недостаточного питания плода
- приобретенная. Формируется под воздействием внешних факторов
- посттравматическая — после травм позвоночника
По форме искривления:
- C-образный сколиоз позвоночника. Формируется одна дуга искривления, позвоночник отклоняется от нормального положения и выпячивается по одной дуге
- S-образный позвоночник. Приобретает форму буквы S, так как к основной дуге присоединяется ещё одна, компенсаторная, направленная в другую сторону
- Z-образный. В позвоночном столбе наблюдают сразу три дуги искривления осанки
По месту локализации:
- шейно-грудной
- грудной
- поясничный
- пояснично-грудной
- пояснично-крестцовый
Статью проверил

Дата публикации: 24 Марта 2021 года
Дата проверки: 16 Февраля 2023 года
Содержание статьи
Причины
Чаще всего торсии — скручивание позвонков — развиваются из-за анатомически неправильного строения рёбер, деформаций межпозвочных дисков и остеохондроза. Также сколиоз возникает из-за:
- стресса, который переносит беременная мать — страдает будущий ребёнок
- неправильной осанки из-за длительной сидячей работы
- онкологических новообразований в спине
- лишнего веса
- травм спины, а иногда даже из-за незначительных ушибов
- неправильного питания и нехватки витаминов
- инфекционных и воспалительных заболеваний
Симптомы сколиоза
I степень. Пациент жалуется на повышенную утомляемость, трудности с поддержанием спины в ровном положении и скованность движений.
II степень. Нарушается осанка и походка, развиваются боли в спине, которые становятся сильнее после нагрузок.
III степень. На этой стадии сколиоза у взрослых и детей появляется рёберный горб. Боль в спине усиливается, конечности часто немеют, беспокоит головная боль и головокружения.
IV степень. У пациента заметно искривлён таз и ассиметрично расположены ноги, развиваются проблемы со стороны внутренних органов.
Степени сколиоза
I степень. На начальном этапе угол деформации позвоночного столба находится в пределах 5⁰. Визуально отклонение заметно, но незначительно. Например, в положении стоя видно, что надплечья находятся на разном уровне, а лопатки — на разной удалённости от позвоночника.
II степень. Угол деформации может доходить до 25⁰. Сутулость хорошо заметна в положении стоя, а при наклоне вперёд появляется ребёрный горб.
III степень. Деформация позвоночного столба доходит до 80⁰. Становится заметной перекошенность таза и всего туловища, деформация грудной клетки.
IV степень. При сколиозе позвоночника в тяжёлой форме деформация превышает 80⁰, все тело пациента становится сильно перекошенным и деформированным. У детей и подростков прекращается рост.
Последствия
Лечение позвоночника наиболее эффективно в детском возрасте. На запущенной стадии можно уменьшить угол искривления и не допустить дальнейшего прогрессирования болезни. Без лечения болезнь прогрессирует и может привести к инвалидности.
Диагностика
Способы выявления сколиоза:
- Визуальный осмотр. Обследование проводят в трёх положениях тела: стоя, сидя и лёжа. Врач измеряет длину ног, изучает подвижность суставов и поясницы, оценивает мышечный тонус, асимметрию позвоночника, таза и грудной клетки
- Рентгенография. Делают несколько раз в год. При этом смотрят снимки при разном положении тела больного, чтобы получить результаты в разных проекциях. С помощью снимков возможно определить угол искривления, а также обследовать состояние позвонков.
- МРТ. Более информативен при патологиях хрящей и мягких тканей.
Лечение сколиоза
Лечение зависит от степени сколиоза. На I стадии искривления лечение направлено на предотвращение дальнейшей деформации. Оно состоит из лечебного массажа спины, грудной клетки и живота, плавания, физиотерапии и гимнастики. На II стадии к перечисленным процедурам добавляют ортопедические корсеты и вытяжение на наклонных кроватях. На III стадии вылечить сколиоз можно только у детей до 11 лет, а на IV — помогает хирургическое лечение.
Массаж при сколиозе
Врачортопед подбирает технику массажа индивидуально. При нем с разной интенсивностью воздействуют на мышцы шеи, ягодиц, ног, поясницы, грудного и крестцового отделов.
Лечебный массаж спины при сколиозе проводят в два этапа:
- Интенсивные техники для увеличения мышечного тонуса и ускорения кровообращения.
- Смягчающие техники, направленные на устранение гипертонуса и общее расслабление тела.
При сколиозе позвоночника важны:
- ритмичные поглаживания вдоль спины
- глубокие поглаживания открытыми ладонями
- вибрация рёбрами ладоней с обеих сторон
- разминание области с высоким тонусом
- круговые растирания пальцами и ладонями
- скольжение фалангами пальцев по спине
- растягивание мышц с гипертонусом
- поглаживания и разминания сосудистых сеток
Дополнительно могут назначить массаж грудной клетки, живота и стоп. Так можно восстановить кровоток по всему телу и снять напряжение.
Корсеты для позвоночника
При сколиозе корсет эффективен только в возрасте до 12 лет. Корректор осанки сдавливает искривлённые области и останавливает деформацию позвоночника. Он фиксирует позвонки в здоровом расположении и снижает уровень нагрузки на больное место.
Также можно использовать бандаж. Он напоминает обычный пояс, который подойдет для профилактики сколиоза. В отличие от жёсткой конструкции корсета, бандаж изготовлен из мягких материалов.
Физиотерапия при сколиозе
Физиотерапевтические процедуры восстанавливают метаболизм и кровообращение, помогают снять или уменьшить боль, воспаления и отёки.
Обычно в физиолечении применяют :
- ультрафонофорез. Он увеличивает биодоступность лекарств при лечении тяжёлых стадий заболевания.
- электронейростимуляцию. Слабый ток воздействует на чувствительные рефлекторные точки тела.
- электрофорез. Снимает боль, спазмы, гипертонус мышц, компрессию нервных волокон.
Мануальная терапия и остеопатия при сколиозе
При лечении сколиоза мануальной терапией у пациентов налаживается работа опорно-двигательного аппарата, а структуры позвоночника принимают физиологически правильное анатомическое положение.
Для лечения искривления осанки применяют:
- разминания
- вытягивания
- скручивания
- растирания
- вибрации
- поглаживания
- постукивания
- сжимания и разжимания
Чтобы процедуры давали нужный результат, нужно:
- ходить на занятия не более 2 раз в неделю
- пройти полный курс мануальной терапии
- комбинировать с физиопроцедурами
- избегать боли и перенагрузки
Кинезиотейпирование
Тейпирование при сколиозе назначают для снятия симптомов. Мышцы спины растягиваются или сокращаются неравномерно, что приводит к болевым ощущениям, нарушениям кровообращения, гипертонусу или мышечной атрофии. Эластичные клейкие ленты равномерно распределяют нагрузку, снимают напряжение и боль, уменьшают тонус и восстанавливают подвижность опорно-двигательного аппарата.
Операции при сколиозе
Хирургическое лечение применяют редко, на 3-4 стадиях или если если другие методы лечения не помогают. Операция по исправлению сколиоза:
- исправляет серьёзные нарушения и деформации позвоночника
- приостанавливает дальнейшее развитие заболевания
- препятствует возникновению осложнений и патологий внутренних органов
- устраняет некоторые косметические недостатки и нарушения
Решение о проведении операции может принять только остеопат. Детям назначают операции только после завершения роста скелета.
Другие методики в лечении
Иглорефлексотерапия. В лечении сколиоза помогает избавиться от боли, гипертонуса, мышечных спазмов и судорог. Также иглоукалывание налаживает кровоток и поступление в организм питательных веществ.
Тракции. Вытяжение позвоночника при сколиозе выполняют на специальном тракционном оборудовании. Тракции направлены на восстановление физиологического расположения позвонков.
Препараты. Медикаментозную помощь при сколиозе назначают в качестве профилактики и поддержания стабильного состояния пациента.
Физкультура. Занятия спортом благоприятно влияют на весь опорно-двигательный аппарат, тренируют мышцы, создают здоровую нагрузку на спину
ЛФК и спорт при сколиозе
ЛФК при сколиозе укрепляет мышцы спины, стабилизирует позвоночный столб, улучшает осанку и работу внутренних органов. Чтобы лечебная гимнастика при сколиозе была полезной, упражнения нужно выполнять только по согласованию с врачом.
При сколиозе назначают следующие упражнения:
- лечь на спину, завести руки за затылок, сводить и разводить локти
- в том же положении поднимать согнутые ноги и подтягивать их к животу
- согнуть ноги и подтянуть стопы так, чтобы они стояли максимально близко к тазу, из этого положения поднимать таз
- лечь на живот и попытаться оторвать вытянутые руки от пола, если получается — вытянутые руки и ноги одновременно
- лечь на живот, опереться ладонями вытянутых рук о пол, на вдохе приподнять туловище над полом
Также следует делать регулярную зарядку. С осторожностью отнеситесь к:
- Бегу. Иногда разрешают бег на 1–2 стадиях, но без резких движений и рывков. После бега не должно быть одышки, боли в спине и ногах и другого дискомфорта. Если бегать больно или сложно, лучше выбрать спортивную ходьбу.
- Плаванию. При сколиозе стоит воздержаться от активного и профессионального плавания. Иначе могут возникнуть осложнения, так как плавание требует высокой подвижности позвоночника.
При сколиозе врачи назначают занятия на турнике для укрепления спины и мышц. Чтобы упражнения принесли пользу, нужно:
- следить за дыханием
- избегать резких движений
- наращивать количество подтягиваний постепенно
- спускаться с турника через стул, без прыжков
Физические нагрузки при искривлении осанки обеспечивают равномерную работу всех структур опорно-двигательного аппарата. Кроме ЛФК и гимнастики можно заниматься йогой. Врач спортивной медицины или остеопат подбирает индивидуальный комплекс упражнений при сколиозе, а также определяет длительность, интенсивность и частоту занятий.
Профилактика
Профилактика сколиоза помогает прежде всего детям. Важно:
- не торопиться с усаживанием ребёнка на первом году жизни — делать это в положенный срок
- для школьника — подобрать удобный рюкзак, письменный стол и стул
- регулярно заниматься волейболом, плаванием и другими видами спорта, полезными для спины
- полноценно питаться, употреблять достаточно витаминов, особенно, витамина D
Чтобы предотвратить врождённый сколиоз у новорожденного, беременной женщине нужно принимать витамин В12 и препараты фолиевой кислоты.
Часто задаваемые вопросы
Что делать, если у ребенка сколиоз?
Если у ребенка сколиоз, покажите его врачуостеопату. Скорее всего он назначит лечебный массаж, оздоровительную гимнастику или мануальную терапию. Вылечить сколиоз самостоятельно нельзя.
Чем опасен сколиоз?
В зависимости от тяжести состояния сколиоз приводит к:
- сутулости
- скованности движений
- сильной боли в спине
- нарушению работы внутренних органов
- асимметрии рук и ног
- образованию межреберного горба
- деформации грудной клетки
При каком сколиозе дают инвалидность?
Риск инвалидности инвалидности появляется на 4 стадии. Деформированные позвонки смещают и сдавливают друг друга, а также соседние мышцы, нервные волокна, кровеносные сосуды и внутренние органы. Как результат головной мозг не получает достаточно кислорода и питательных веществ, что сказывается на умственных способностях.
Как правильно спать при сколиозе?
Поза во сне при сколиозе зависит от стадии, стороны деформации и локализации болезни. Оптимальный вариант для любого случая — сон на спине, при этом поверхность постели должна быть идеально ровной и твёрдой.
Как выбрать матрас и подушку при сколиозе?
На ранних стадиях или в качестве профилактики болезни можно спать на матрасе средней жёсткости. Со 2 стадии врачи рекомендуют спать на ровном жёстком ортопедическом матрасе. Подушку следует выбирать в форме буквы «П»: по краям высокую и плотную, в центре — более низкую и мягкую.
Источники
«Функциональные методы лечения сколиоза у детей», В. В. Бутуханов, Е. В. Бутуханова. Гений ортопедии, 2003.
«Сколиоз», М.Т. Сампиев, А.А. Лака, Н.В. Загородний. ГЭОТАР-Медиа, 2008.
Статью проверил

Публикуем только проверенную информацию 
Размещенные на сайте материалы написаны авторами с медицинским образованием и специалистами компании ЦМРТ
Подробнее

Понравилась статья?
Подпишитесь, чтобы не пропустить следующую и получить уникальный подарок от ЦМРТ.
Нажимая на кнопку, я принимаю соглашение на обработку моих данных.
![]()
Записаться в ЦМРТ
Нужна предварительная консультация? Оставьте свои данные, мы вам перезвоним и ответим на все
вопросы
